Internal Assessment for 2011 International Review - CIHR Institute of Circulatory and Respiratory Health
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures
- Figure 1: Reduction in coronary artery disease deaths in Canada attributable to risk factor management and treatment advances nationally
- Figure 2: Percentage of total CIHR expenditures related to ICRH mandate over time
- Figure 3: Relative change in number of cardiovascular clinical trials publications since 1997 on an annual basis, comparing top 10 countries
- Figure 4: Specialization index and average of relative citations for top 10 countries publishing cardiovascular clinical trials, 2000–2008
Mandate and Context
Background and overview
The Institute of Circulatory and Respiratory Health (ICRH), one of the 13 institutes at CIHR focusing on health and disease of major organ systems, has within its mandate the organization's largest burden of chronic diseases – including atherosclerosis, heart failure, stroke, asthma, sleep apnea and chronic obstructive pulmonary diseases. This epidemiological reality and the extraordinary diversity of these medical conditions present a daunting research challenge.
Our mission is to support research into the causes, mechanisms, prevention, screening, diagnosis, treatment, support systems and palliation for a wide range of conditions associated with the heart, lung, brain (stroke), blood vessels, blood, critical and intensive care and sleep. Our mandate, which is equally broad, is to engage the research community and encourage interdisciplinary, integrative health research that reflects Canada's emerging health needs. Our mandate further encourages facilitating partnerships and accelerating the transfer of new knowledge into benefits for Canadians.
In 2000, CIHR's grant-funding budget for the ICRH community was $59 million per year and had increased to more than $137 million per year by 2009. Through the Institute's efforts to coordinate strategic partnerships among governmental, academic, private and volunteer sectors,
ICRH has helped stimulate and inspire its various communities; accordingly, CIHR strategic grant expenditures in areas relevant to the ICRH mandate increased from $3.6 million per year in 2000 to $33.7 million per year in 2009,
providing dramatically increased funding for new research programs, multidisciplinary teams, national research networks and international collaborations.
A time lag exists between research discovery and health impact (our current estimate is 12 to 15 years). Therefore, ICRH has put emphasis on anticipating the potential future challenges in health needs by facilitating long-range solutions and collaborations. Taking advantage of scientific advances, ICRH has provided leadership integral to the development of the Canadian Heart Health Strategy (2008), the National Lung Health Framework (2009), and the National Sodium Reduction Strategy (2010). With the launch of knowledge translation (KT) programs and high profile chairs, we and our partners contributed to and supported recent major advances in circulatory and respiratory conditions, including the highest rates of hypertension controlFootnote 1,Footnote 2 and the lowest rates of smoking among western countries.Footnote 3
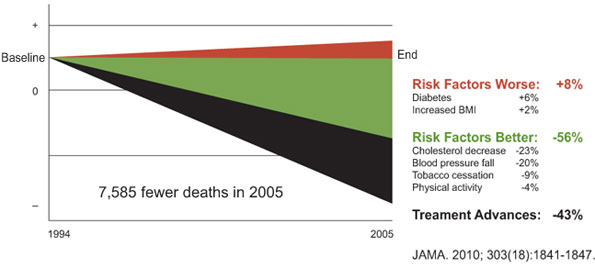
ICRH efforts will help accelerate these important advances and contribute to the already observed decreased mortality and age- and sex-adjusted incidence of chronic heart and lung diseases in Canada (Figure 1).Footnote 4,Footnote 5
Figure 1: Reduction in coronary artery disease deaths in Canada attributable to risk factor management and treatment advances nationallyFootnote 4
International perspective
Globally, chronic diseases, including circulatory and lung diseases, are evolving to be the number one health burden for both high and middle income countries.Footnote 6 It is projected that over the next 20 years, circulatory and respiratory diseases will become the major killers in populous middle-income countries such as China, India and Brazil.
Despite Canada's relatively small population (3% of world population), Canadian researchers contribute 6% of the research output in the cardiovascular clinical trials field. Although Canada has the smallest population of the G7 countries, and one of the most modest research budgets, its cardiorespiratory research output is on par with that of Japan, Germany, the United Kingdom and France. The number of publications is about one-fifth that of the U.S. even though Canada's population is less than one-tenth and the CIHR's grant budget for the ICRH community is only about one-twentieth that of the National Heart, Lung and Blood Institute (NHLBI) research budget ($137 million versus $2.9 billion per latest fiscal year). More importantly, the quality of Canadian-led publications is highly regarded.Footnote 7
ICRH has worked closely with its international partners to support research innovation and application. Despite a relatively modest budget (the total annual strategic budget for the Institute being stable at $8.5 million), ICRH was able to partner effectively with the NHLBI on three ongoing major bilateral programs (Resuscitation Outcomes Consortium, Cardiothoracic Surgical Network and Heart Failure Network). For these programs, the ICRH total contribution per program over five years is in the range of $2.5 to $5 million, for a total combined program budget of $35 to $55 million. The Canadian contributions are particularly appreciated for the innovative research proposals, efficiency in research execution and high quality data and outcome capture. ICRH also partners with European and Asian research agencies (e.g., the Finnish Funding Agency for Technology and Innovation and the National Natural Science Foundation of China) for major collaborative research programs.
Incorporation of recommendations from the 2006 International Review
Comments from the 2006 International Review report panel for ICRH, which included Dr. Jeffrey Drazen, editor of the New England Journal of Medicine, noted the overall excellent performance of the Institute, with particular credit given to the Scientific Director, Dr. Bruce McManus, for guiding ICRH through its establishment. While basic science research was regarded as vibrant, other research themes were identified as needing growth. Also noted were a lack of coordination between health funders and health researchers, and challenges faced by young investigators entering health research. Finally, reviewers identified that important research opportunities in the areas of sleep, blood and lung diseases needed to be explored more fully.
In response to the International Review, ICRH made a number of strategic decisions to address these issues. To provide balance across the four CIHR pillars,
ICRH has focused on enriching clinical research by developing new clinical research networks.
In addition, it has expanded its mandate for outcomes research. By facilitating and subsequently serving on the steering committees of the Canadian Heart Health Strategy and the National Lung Health Framework, the Institute coordinated the translation of research evidence into clinical practice and health systems changes. Finally, ICRH has developed capacity-building programs and special initiatives to encourage and enrich the smaller research communities – a move to which the communities have responded enthusiastically.
Institute Priorities
At the inception of CIHR, ICRH faced significant challenges. In 2000, circulatory diseases were the number one killers of Canadians (accounting for 37% of mortality, or 75,000 deaths per year). Lung disease was the third highest cause of death (10% of mortality, or 18,000 deaths).Footnote 8,Footnote 9,Footnote 10 The challenge was further compounded by the large economic burden associated with circulatory and respiratory diseases.
Since 2000, ICRH has worked closely with the research community, partners and other stakeholders to identify gaps, needs and emerging opportunities. It has undergone two major consultation processes – one soon after its inception and another in 2006. Each time, the process identified new priorities and/or modified existing strategic directions. Following the 2006 International Review, the Institute also made revisions to its initial strategic programs so that it could serve the ICRH community better. A new set of strategic consultations was initiated in 2010 in anticipation of the next phase of development at ICRH and the International Review in 2011.
ICRH strategic priorities for 2000–2005
During the Institute's early years, under the leadership of Dr. McManus, its priorities focused on expanding its research mandate in the heart, lung and blood domains. This included expanding research programs beyond basic science research to clinical, health services and psychosocial dimensions.
Following consultation with numerous stakeholders and partners, ICRH developed its first strategic plan in 2002–2003. The following areas were identified as examples of high importance:
- Interaction of genes and environment in determining susceptibility to circulatory and respiratory diseases
- Influence of sex and gender on the risk of cardiovascular disease
- Regeneration, repair and replacement of damaged cells, tissues and organs
- Obesity-associated vascular and respiratory conditions
- Altering the disease consequences of cystic fibrosis
- Training initiatives
- Legal and ethical issues in circulatory and respiratory research
ICRH strategic priorities for 2006–2010
Following the 2006 International Review of CIHR and the appointment of a new Scientific Director, Dr. Peter Liu, the Institute underwent a second priority-setting exercise, building on the successes of the inaugural director.
The ICRH Institute Advisory Board (IAB), together with the community and partners, identified the escalating burden of chronic diseases in the ICRH domain as the key future challenge. With advancing age and increasing prevalence of risk factors such as obesity, diabetes and hypertension in our population, we are increasingly faced with chronic circulatory and respiratory complications such as heart failure, stroke-related disabilities, asthma and chronic obstructive pulmonary diseases and associated co-morbidities.Footnote 11,Footnote 12 The Institute also recognized the important contributions of sleep disorders to chronic vascular, respiratory, metabolic and neurological conditions. The strengths of research in blood and coagulation, critical care and stroke were recognized internationally but required ICRH-led coordination.
To address the challenges of chronic diseases, the IAB, working with the ICRH research community, identified the following priorities:
- Understand the upstream factors that contribute to chronic heart and lung diseases including diabetes/obesity, at-risk behaviours, inflammation and sleep disorders, and seek appropriate solutions
- Identify individuals at risk of complications by identifying earlier presence of the disease through biomarkers, imaging or risk stratification strategies
- For those with existing complications, develop strategies to deliver coordinated, effective care (e.g., improve resuscitation outcomes, regenerate rather than palliate and advance personalized care)
To achieve these goals, it was necessary to build multidisciplinary teams, networks and consortia, in addition to nurturing the smaller ICRH research communities such as those associated with sleep, blood, lung and critical care. For each of these priorities, we developed customized programs or targeted requests for applications (RFAs) to build capacity and research collaboration.
In addition, the Institute recognized the importance of providing a more efficient interface between researchers and knowledge users, coordinating diverse efforts to address the challenges of circulatory and lung disease, and engaging various stakeholders for circulatory and lung research. To achieve this,
ICRH had the unique opportunity of working closely with the federal and provincial governments to propose, develop and launch national strategies in circulatory and respiratory diseases,
namely the Canadian Heart Health Strategy and Action Plan, the National Lung Health Framework and the National Sodium Reduction Strategy.
These strategies were supported by the federal government and multi-sectoral stakeholders with major strategic input and leadership provided by Dr. Liu. Dr. Liu worked closely with volunteer health agencies, professional organizations, various governmental agencies (e.g., Health Canada, Public Health Agency of Canada and Industry Canada) and academic researchers, and participated in executive or steering committee roles.
ICRH is the only CIHR Institute that has co-led three major national health and knowledge translation strategies in the past five years.
ICRH strategic priorities beyond 2010
With the launch of CIHR's Roadmap for research in 2009 and the successful launch of many of the strategic initiatives set out in ICRH's 2006 strategic plan, we recently updated the strategic plan for 2010–2012, providing a guide for ICRH activities until completion of the 2011 International Review. With the anticipated transition of the Institute's scientific director, this will ensure that ICRH is in the strongest possible position to embrace the change.
Key Initiatives
Unique ICRH integrated program delivery model for strategic initiatives
Each of the major initiatives launched by ICRH since 2006 is matched to a strategic priority of the Institute and incorporates an integrated program delivery model designed to achieve the initiative's goals – including knowledge translation (KT) and training – in a coordinated fashion. For example, for each major initiative we sought funding and knowledge translation partnerships with governmental, volunteer and private sectors ahead of launch. In addition, for each ICRH program we implemented a process by which funded research teams and trainees meet regularly to report on their scientific progress with feedback from an external advisory panel. This process not only ensures robust progress and accountability but also promotes further excellence, encourages collaboration and maximizes interdisciplinary training. Moreover, to maximize integrated KT, ICRH also made efforts to ensure that annual reporting and advisory sessions coincided with major national or international scientific meetings, allowing funded teams to profile the program's research findings as well as promote public engagement through Café Scientifiques.
This model has enabled ICRH to create interactive research communities that have sustained impact beyond that of their individual research projects.
Due to space limitations, we will profile only a few initiatives as examples of our Institute's novel approach to creating unique virtual research communities.
Initiative 1: Diabetes and cardiovascular complication
Diabetes and its associated risk factors, including obesity and hypertension, have evolved as a critical rising health burden for Canada. Therefore, ICRH designated cardiovascular complications of diabetes (CVD-Diabetes) as a high priority strategic initiative.
The Institute held a national workshop in June 2005 to define the priorities and scope of associated programs. In February 2006, ICRH launched an integrated program in CVD-Diabetes, offering seed grants (two-year funding) and team grants (five-year funding), in partnership with CIHR's Institute of Aboriginal Peoples' Health, Institute of Infection and Immunity, and Institute of Nutrition, Metabolism and Diabetes (INMD). These are joined by significant contributions and partnerships from the Canadian Diabetes Association (CDA), Heart and Stroke Foundation of Canada (HSFC), Pfizer Canada, Finnish Funding Agency for Technology and Innovation (Tekes), Health Canada and in-kind contributions from the National Institutes of Health (NIH). The objective of the team grants was to strengthen Canadian and international health research in the area of diabetes and link it to cardiovascular complications; specifically, the focus of the multidisciplinary team grants was on basic innovations in understanding disease mechanisms and on linking these to novel therapeutic or prevention approaches.
The Institute invested an initial $5 million over five years into the CVD-Diabetes program. However,
ICRH leveraged more than $19.8 million in partner funding for the support of research teams,
including an investment of $10.4 million from Tekes, $2.5 million from Pfizer, $650,000 from HSFC, $500,000 from CDA and $900,000 from INMD – on top of the Institute's initial contribution. The partnership with Tekes is a key international collaboration. The most recent Newsweek ranking (August 2010) of countries for innovation in the 21st century identified Finland as number one in the world (Canada is seventh and U.S. is 11th), mainly because of its national innovation strategy. Tekes is the Finnish funding agency for technology and innovation for the entire country and is partnering with our Institute on a number of key initiatives.
The Institute received many applications in response to the CVD-Diabetes RFA, resulting in three seed grants and three teams approved for funding. All successful teams were multidisciplinary or interdisciplinary in nature, including:
- Dr. Richard Gilbert – Dysfunctional endothelial cell repair in diabetes: pathogenetic mechanisms and regenerative strategies, investigating novel mechanisms and therapies for diabetic vascular disease
- Dr. Robert J. Petrella and Finnish teams – Innovation to reduce cardiovascular complications of diabetes at the intersection of discovery, prevention and knowledge exchange, identifying precise strategies to address microvascular to macrovascular investigation using animal and human models
- Dr. André Marette and Finnish teams – Cardiovascular complications in type 2 diabetes: genetic and metabolic determinants from mouse to man to population, investigating genetic determinants of diabetes and its complications, and the functions in unique animal models of diabetes-linked atherosclerosis
The collaborating Canadian and Finnish teams are perfect complements to each other and together are achieving insights not possible when acting alone.
Initiative 2: Advances in imaging and early disease detection
In 2006, following extensive consultations, ICRH with its partners and stakeholders identified technology for diagnostic and therapeutic advances, including imaging technologies for early detection of disease, as one of ICRH's top priorities. Imaging has been one of the top medical advances in the past decade. Innovations in imaging have continued to emerge at an astounding pace, creating the potential for earlier, less invasive and more accurate diagnosis of circulatory and lung diseases and the opportunity to improve health outcomes substantially.
To identify the key gaps and opportunities for research and knowledge translation in this area, ICRH hosted a workshop (March 30–31, 2007), inviting broad participation from national and international imaging scientists, molecular biologists, clinicians, epidemiologists, policy makers, partners and industry representatives. There was a vigorous exchange of ideas, with all parties agreeing that fast-tracking clinical applications of innovation – and, as such, maximizing their impact on clinical decision making – would help make Canada a world leader in this domain.
The report from this initiative formed the foundation of the Clinical Imaging Team Grant Request for Applications (RFA) that ICRH launched in June 2008 with other institutes and partners. The applicants were asked to address the critical steps between technology development, clinical implementation and clinical decision making.
The aim of the program was to build an integrated platform that would enable the conduct of methodologically sound, policy-relevant outcome trials that objectively establish the role of new imaging technologies.
The Institute received 11 letters of intent and eight parties were invited to submit an application. Following peer review, the top four applications were approved for five-year funding in partnership with Tekes and the HSFC for an estimated total investment of $10.8 million (ICRH $8.1 million, HSFC $1.25 million, Tekes about $1.4 million).
Initiative 3: Building new networks in clinical research, including rapid response
One of ICRH's unique goals was to create a forum to link Canadian centres of excellence in research and patient populations into effective networks for clinical evaluation and to promote the translation of basic innovations into clinically useful tools. Canada has the advantage of being noted for clinical epidemiology and evidence-based medicine, with a nationalized health care system that facilitates long-term patient outcome capture. In addition,
ICRH was the champion of the Clinical Research Initiative at CIHR, leading the charge to develop a framework for initial pilot models that would strengthen clinical research in Canada.
To foster excellence and expand clinical research in Canada, ICRH invested strategically in Clinical Research Networks focused on research excellence and global impact. ICRH initiatives prompted the research community to develop successful applications that led to the funding of several major clinical research networks, including:
- The Canadian Atherosclerosis Imaging Network led by Dr. Jean Claude Tardiff and other centre investigators – now a tour de force in cardiorespiratory imaging research
- A global trials network, the Canadian Network and Centre for Trials Internationally, led by Dr. Salim Yusuf at McMaster University and Dr. John Cairns at the University of British ColumbiaFootnote 13
- The Canadian Cohort of Obstructive Lung Disease led by Dr. Jean Bourbeau from Université Laval, which received matching funding from CIHR and the private sector to study the new epidemiology of chronic obstructive pulmonary disease
- Continued support of the very productive Canadian Cardiovascular Outcomes Research Team, led by Dr. Jack Tu
The latter team produced the Canadian Cardiovascular Outcomes Atlas and has published major articles in the New England Journal of Medicine, the Journal of the American Medical Association and Circulation on the impact of clinical practice, health policy and health systems on cardiovascular outcomes.
ICRH played a strategic role in the development and success of these clinical research networks by facilitating, advising, partnering or launching funding opportunities.
Finally, during the onset of the H1N1 pandemic in 2009, Canada was faced with an unprecedented number of young patients dying of respiratory illness in intensive care units.
ICRH worked with the research community to launch an ultra-rapid research grant that facilitated collaboration among critical care centres in Canada and globally.
These networks developed a pilot clinical trial to evaluate novel anti-inflammatory treatments for affected patients – the InFACT Network.Footnote 14 Inception of the research idea, development of the RFA, approval through CIHR's Scientific Council, launch of the RFA, review and actual award of the grant took a record six weeks.
Initiative 4: Resuscitation Outcomes Consortium
The Resuscitation Outcomes Consortium (ROC) is a unique international clinical research network conducting research in cardiopulmonary arrest and traumatic injury leading to arrest. ROC is a joint international collaboration among the National Heart, Lung and Blood Institute (NHLBI), ICRH, HSFC, Defence Research and Development Canada, U.S. Department of Defence and the American Heart Association. ICRH has been an integral and enabling partner since its inception, providing research input, partnership funding and team participation for six years. The ROC network consists of nine regional clinical centers (RCCs) and one data coordinating centre. There are two composite Canadian teams: the Toronto Regional Coordinating Center and Ottawa-Ontario Prehospital Advanced Life Support Study-British Columbia RCC. The Canadian teams are the leaders in recruitment, important substudiesFootnote 15 and setting standards in ethics.Footnote 16
The ROC program is funded through NHLBI and its partners for a total of $45 million over six years, with ICRH contributing $3 million over the first six years (up to 2010). In 2009, the ROC passed a rigorous NIH review and renewal process and was awarded new funding to 2016.
The ROC network represents a breakthrough model in developing an ethical research framework, including randomized trials in a pre-hospital setting through an international collaboration.
The ROC is the first and only large-scale effort in the world to conduct clinical trials that focus on the very early delivery of interventions by emergency medical services teams in the field where critically ill patients are first contacted and where there is the greatest potential for patient benefit from immediate intervention. ROC has made outstanding progress in setting up essential infrastructure, defining new standards for quality of CPR monitoring during resuscitation and applying rigorous standards to carry out Emergency Medical Services research.
Outputs and Outcomes
Overall, the research communities at ICRH are extremely active in generating research and translating research into revised clinical guidelines, reformed practices, changes in health policies and systems and improved health outcomes. As depicted in Figure 2, since 2000, the ICRH research community has kept up with CIHR growth, maintaining its proportion of total CIHR expenditures across all open funding streams. Grant expenditures (open and strategic competitions) in areas under the ICRH mandate increased from $59 million in 2000–2001 to $137 million in 2009–2010. Similarly, investment in training support (open and strategic) has increased from $6 million in 2000–2001 to $11 million in 2009–2010. Although the number of senior investigators in the ICRH community with salary support from CIHR has diminished with time, funding for salary support in both open and strategic competitions remained relatively stable, fluctuating between $5.8 million (2000–2001) and $5.2 million (2009–2010).
Figure 2: Percentage of total CIHR expenditures related to ICRH mandate over time
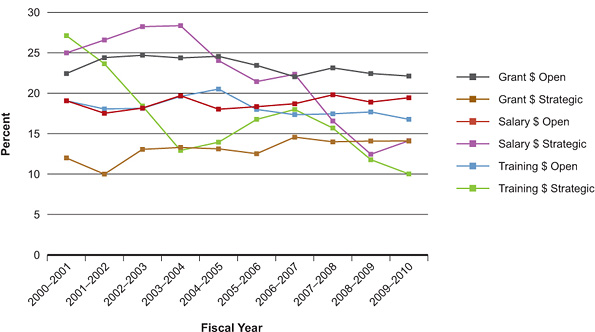
In line with federal policy, senior investigator funding was diverted into the Canada Research Chairs (CRC) program. As such, CRC funding towards ICRH-related research increased from $432,000 to $801,000 from 2005–2006 to 2009–2010. This increase may help explain the drop in CIHR expenditures towards strategic salary awards for investigators, mid-career investigators and distinguished scientists for ICRH-related research and CIHR as a whole. It must be noted that funding data were based on a keyword search of the CIHR funding database and validated through a subjective process. Projects may have multiple institute affiliations.
Advancing knowledge
The ICRH research community has been very active over the past five years, producing top-quality publications that have contributed significantly to the world literature in the areas of heart, lung, blood and critical care research.
As an example, the ICRH community led 23 original research articles published from 2006 to June 2010 in the New England Journal of Medicine – one of the highest impact medical journals worldwide (Impact factor >35). This represented 40% of all publications from Canada in this prestigious journal during this time period.
These are Canadian-led international studies, including early versus late intervention for acute myocardial infarction (transfer-MI,Footnote 17 TIMACSFootnote 18), anticoagulation in acute coronary syndrome;Footnote 19 darbigatran vs. warfarin (RELY),Footnote 20 clopidogrel vs. aspirin,Footnote 21 or rhythm vs. rate control for atrial fibrillation (AF–HF),Footnote 22 ramipril in prevention of diabetes (DREAM),Footnote 23 epidemiology of diastolic heart failure,Footnote 10 effectiveness of drug eluting stents,Footnote 24 link between medication use and policy,Footnote 25 mepolizumab,Footnote 26 bronchial thermoplasty for asthma control,Footnote 27 and ROC publications.Footnote 15,Footnote 16 Many of these publications are landmarks in their respective fields, setting new directions in research or having major impacts on clinical practice or health system delivery. These impacts build on the existing excellence in basic science research cited as one of ICRH's strengths in the 2006 CIHR International Review.
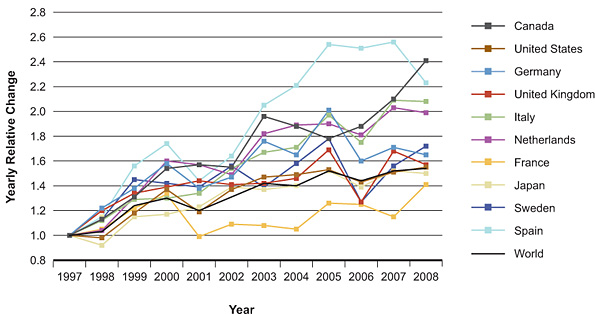
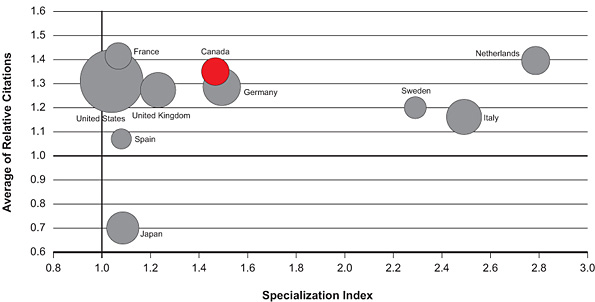
ICRH's efforts in promoting clinical research, including funded research networks, partnered consortia and support of young investigators, have contributed to an increase in the number of publications for clinical trials in ICRH domains. The publication number has more than doubled in the last 10 years and is among the highest in the G20 countries (Figure 3). As shown in Figure 4, Canada scores above the world average (1.0) on both the average relative citation, or ARC (1.35) and the specialization index, or SI (1.46) for publications in the area of cardiovascular clinical trials for 2000–2008. Furthermore, Canada ranks third among the top 10 countries for ARC, closely behind France (1.42) and Netherlands (1.40). Publications on cardiovascular clinical trials were identified through U.S. National Library of Medicine Medical Subject Headings searches done by the Observatoire des Sciences et des Technologies. Databases searched may not cover all publications in this area and ARC data is incomplete for 2008. Countries were ranked based on total number of publications (2000–2008). Many investigators among the ICRH research community are international leading-edge researchers. For example, Dr. Salim Yusuf was among the top 10 highest cited researchers in all of scientific research in 2008, according to Science Magazine, and has been cited more than 13,365 times in the last decade. And he is just one among many.
Figure 3: Relative change in number of cardiovascular clinical trials publications since 1997 on an annual basis, comparing top 10 countries
By identifying research priorities and launching specific and targeted programs,
the Institute has had a major role in promoting and supporting research in some of the traditionally smaller ICRH research communities, including respiratory, blood and sleep domains.
Over the past few years, we have observed a direct increase in the number of successful research projects and the total funding amounts from CIHR and ICRH to these communities. For example, the levels of activity in the blood and sleep domains were modest to negligible at the beginning of 2000. These have grown dramatically over the past decade, particularly in the last five years with ICRH engagement and encouragement. Specifically, funding in the area of blood research has increased in the open competitions (from $2.1 million in 2000–2001 to $14.1 million in 2009–2010) and strategic competitions (from $0.03 million in 2000–2001 to $3.2 million in 2009–2010). Similarly, funding of respiratory research has increased in the open grant competitions (from $12.6 million in 2000 to $24.7 million in 2009–2010) but particularly in the strategic initiatives (from $0.3 million to $8.8 million over the same period). A current initiative in sleep research led by ICRH will have a similar impact on this community in the future.
Figure 4: Specialization index and average of relative citations for top 10 countries publishing cardiovascular clinical trials, 2000–2008
CVD-Diabetes Initiative
The CVD-Diabetes initiative created a new research consortium among the teams that fostered stronger national and international collaborations through co-supervision of students, staff exchange, co-funding and co-management of collaborative projects. Moreover, the creation of the CVD-Diabetes network provided means for nurturing numerous new collaborations between funded teams (e.g., Drs. André Marette and Richart Gilbert) as well as with new investigators (national and international) outside this program. To date (July 2010), the CVD-Diabetes Initiative has supported 27 graduate students and 13 postdoctoral fellows. The numerous publications (more than 100), conference proceedings and abstracts (more than 200) published to date as a result of this funding opportunity attest to the success of the initiative and the dedication of all teams to collaborative work and research excellence. Knowledge translation (KT) has also been an integral part of this program from its inception, moving knowledge from discovery into practice, programs and policy. For example, Dr. Robert Petrella's team is developing best practices for the prevention and reversal of cardiovascular complications at the point of care – practices that have been adopted by the Ontario Ministry of Health. Dr. Gilbert's team has filed provisional patents for new treatments for diabetic nephropathy and heart failure, and has initiated a clinical study evaluating the effects of autologous endothelial progenitor cell therapy in patients with diabetic nephropathy. Lastly, Dr. Marette's team recently established a collaboration with Rigel Inc., a U.S. pharmaceutical company, to jointly develop mimics of adiponectin to limit cardiovascular complications in diabetes.
Clinical imaging initiatives
Prior to ICRH, the clinical imaging community was disparate and dispersed in Canada. ICRH's imaging initiative coalesced the community into a major national imaging network to evaluate novel diagnostic imaging technologies and establish their applications in clinical settings. The Canadian Atherosclerosis Imaging Network (CAIN) is a pan-Canadian imaging network funded through grants from CIHR ($2 million per year for five years) and the Canada Foundation for Innovation. CAIN is conducting cross-sectional and longitudinal clinical imaging studies of atherosclerosis in coronary, carotid, peripheral and pulmonary vascular beds. Vascular imaging expertise and infrastructure in all major Canadian centres are linked in this novel multidisciplinary research network. CAIN has been successful in training clinician-researchers, generating standardized imaging protocols across the country and promoting young investigators' protocols involving 40 investigational sites and 120 individuals.
CAIN has also established collaboration with the International Partnership for Critical Markers of Disease, allowing CAIN to disseminate information about its experts' work to a broad audience that includes key national and international governmental, industry and academic leaders.
CAIN also engages key regulatory agencies, including Health Canada, the U.S. Food and Drug Administration and the European Medicines Agency, and works along with pharmaceutical and biotechnology discovery teams. Recently, CAIN established collaborations with Hoffmann-La Roche, resulting in additional funding of more than $50 million into the network. To further support the clinical imaging community, ICRH funded four additional teams in partnership with the Heart and Stroke Foundation of Canada (HSFC) and the Finnish Funding Agency for Technology and Innovation to develop innovations in imaging.
Similar to the CVD-Diabetes program, ICRH is maintaining close links with the imaging research community, providing further support as needed and closely monitoring progress through annual reporting and advisory sessions. As strengths are built around the cardiorespiratory imaging community, its members have leveraged success upon success. For example, in June 2009, ICRH partnered with the Institute of Cancer Research and four other CIHR Institutes and the Natural Sciences and Engineering Research Council of Canada to fund research that will accelerate the development of alternatives to 99mTc radiopharmaceuticals. Remarkably, five of the seven fundable projects submitted were from the ICRH community. ICRH will invest more than $850,000 for this program with significant leverage. Most recently, the Government of Canada earmarked in its 2010 budget an additional $10 million to build excellence in imaging clinical-trial networks. ICRH is an active participant in discussions that focus on developing future programs in this research area. The Institute's imaging networks will form a backbone that will fast track innovation to application for other domains in the research community.
Capacity building
Over the past few years, the number of ICRH researchers and research activity associated with the Institute have both increased. To encourage continued capacity building in ICRH-relevant fields, the Institute has engaged in a number of strategies with the research communities, with the goal of enhancing the success of established researchers and encouraging young investigators to enter ICRH-relevant research areas. Further, in recent years ICRH has put special emphasis on working closely with the smaller ICRH research communities and volunteer health organizations to support research and training in domains such as sleep, critical care, blood, pulmonary and stroke. These partnerships have included support of training awards with the Canadian Sleep Society, Canadian Critical Care Trials Group, HSFC, Canadian Blood Services and the Canadian Thoracic Society–Canadian Lung Association. ICRH team members attend numerous research community and network meetings offering strategies and encouragement for grant applications.
Trainees and young investigators in ICRH communities
Training of young investigators and graduate and postdoctoral fellows has been a major priority for ICRH. The most important young investigators program that ICRH has invested in over the past five years is the Strategic Training Initiative in Health Research (STIHR) program. ICRH funded 12 STIHRs, supporting more than $15 million over six years for young investigators in areas such as interdisciplinary heart and lung research, transplantation, inflammation, public health, structural biology and regenerative medicine. In the most recent renewal rounds, ICRH funded three of the STIHR programs, two of them focusing on pulmonary diseases. An earlier survey indicated that upon completion of their research training, the vast majority of trainees funded through STIHR (85%) plan or have found a career in health research.
Young investigator training events and workshops
Since 2004, ICRH has held an annual Young Investigators Forum in various cities across the country to engage graduate students, postdoctoral fellows and young investigators with senior mentors and role models. This mechanism also facilitated young investigators to further build their careers in research and develop leadership skills. Each year, about 150 to 250 young investigators attend this event to network, explore interdisciplinary research, interact with peers and mentors and showcase their research in competitions. Invited keynote speakers included Dr. Elizabeth Nabel (Director, NHLBI), Dr. Valentin Fuster (President, World Heart Federation) and Dr. Luis Ignarro (Nobel Prize winner). The forum is one of ICRH's flagship programs, receiving excellent feedback and vigorous participation.
Programs supporting research chairs and clinician-scientists
In addition to the Canada Research Chairs program for senior investigators, ICRH has continued to support select chairs for designated purposes. One example is the CIHR Chair in Hypertension Prevention and Control, created in partnership with HSFC and focused on KT and health policy implementation. Dr. Norm Campbell, the most recent recipient, has been instrumental in changing hypertension screening and treatment in Canada as a result of this chair.Footnote 1,Footnote 2 ICRH also partnered with the CIHR Institute of Population and Public Health on the Public Health Chairs program, supporting a Public Health Research Chair in Chronic Diseases Prevention. In addition, ICRH supported a number of clinician-scientist awards, recognizing the challenges in building successful careers in the current environment. In view of CIHR's new Roadmap priority of patient-oriented research, the clinician-scientist should become a major area for future investment.
ICRH partners' forum
To build capacity in the ICRH community on selected topics, ICRH held a biennial Partners' Forum. In 2007, the Institute hosted a workshop to raise awareness of and build capacity in KT science. The workshop provided participants with an opportunity to network with stakeholders and partners. Another KT workshop was hosted by ICRH in 2009 and focused on applied KT within two domains: clinical practice guidelines and the commercialization of medical technologies. The former focused on state-of-the-art clinical practice guidelines and implementation science, while the latter included stakeholder engagement to identify barriers and facilitators for commercialization of basic biomedical discoveries.
Informing decision making
Canadian Heart Health Strategy
In 2006, Dr. Liu, representing ICRH, together with the Canadian Cardiovascular Society, HSFC and Dr. Eldon Smith from the University of Calgary, obtained support from the Honourable Stephen Fletcher, Parliamentary Secretary of Health and the Honourable Tony Clement, Minister of Health, to develop the Canadian Heart Health Strategy and Action Plan (CHHS-AP). The CHHS-AP is a comprehensive stakeholder-driven strategy to reduce the growing burden from cardiovascular and cerebrovascular diseases in Canada. It integrates research and knowledge and translates recent important research findings into a major strategic policy proposal to improve health for Canadians from both the population and individual perspectives. The CHHS-AP proposes a six-point plan to reduce risk factors, lower health care costs and ensure Canadians live longer and healthier lives. It is to be implemented in partnership with provincial and territorial health ministries.Footnote 28 A number of ICRH-led research initiatives and KT programs such as Canadian Cardiovascular Harmonized National Guideline Endeavour (C-CHANGE), described below, are based on recommendations stemming from the CHHS-AP.Footnote 28
National Lung Health Framework
ICRH is one of the founding partners of the National Lung Health Framework and is represented on the executive committee. This national strategy is supported by a $10 million federal government start-up implementation fund and by participation from multiple partners, including provinces and territories. The National Lung Framework is a made in Canada action plan developed by and for a wide range of stakeholders working to improve lung health for all in Canada. It is focused on a collaborative approach to the prevention and management of respiratory disease, again aiming to translate research into practice and policies.Footnote 29 Additional funds to support the Framework's goals became available through a partnership between CIHR and Public Health Agency of Canada (PHAC). This program will focus on community intervention research to identify the best policies and implementation science for maximizing lung health in disadvantaged communities.Footnote 29
National Sodium Working Group to reduce sodium for Canadians
ICRH is also a member of the steering committee of the National Sodium Working Group headed by Health Canada with many other stakeholders. The objective of the working group is to reduce the sodium content of foods in Canada and the burden of cardiovascular and other chronic diseases related to excessive sodium intake. The current Canadian diet contains an average of 3,500 mg of sodium per day, while the physiological requirement is only around 1,500 mg per day. Following careful deliberation, Canada set an intermediate target of 2,300 mg maximum sodium ingestion per day to be achieved by the year 2016.Footnote 30 This will be accomplished by a three-pronged strategy including public education, reducing sodium in the food supply and research and innovation. ICRH is the lead Institute for the research prong and Dr. Liu has been the chair of the research subcommittee leading this effort. Several research programs have been launched in partnership with the CIHR Institute of Nutrition, Metabolism and Diabetes and other CIHR partners, together with PHAC, Health Canada and HSFC.Footnote 30
Ethics of public-private partnerships
Ethics of public-private partnerships (PPP) have become an important consideration in many ICRH programs and activities as PPP are often essential. For example, researchers and institutions need guidance on how to make decisions in partnering with the private sector and on how to engage industry effectively and ethically in partnerships for research and knowledge translation. ICRH participated in the development of the CIHR Private Sector Partnerships Ethics Framework, and an ICRH representative is a member of the Working Group on CIHR Ethics Guidelines for Public-Private Partnerships. ICRH also provided key input into the updated version (soon to be released) of the Tri-Council policy statement on the ethical conduct of research with humans.
In addition, ICRH has actively led ethics initiatives in the following areas:
- Integration of an ethics component into the Clinical Imaging Program through a focus on ethics and PPP within the context of the commercialization of imaging technologies (workshop held in April 2009)
- Integration of guidelines on ethics and conflict of interest into PPP of multi-sectoral requests for applications
- Development and implementation of a framework for activities related to ethics and conflict of interest in the national harmonized guidelines endeavour
Café Scientifiques
ICRH has sponsored or partnered on eight Café Scientifique events over the past four years in various locales across Canada. The Cafés provide outreach to the public about current research. They also help health consumers make informed decisions about health and health care. Cafés hosted by ICRH have included titles such as: Air Quality and Your Health, (Toronto), Sleepless in Niagara (Niagara-on-the-Lake), Urban Heart Health (Kitchener-Waterloo), Quand m'entraîner marrette de respirer! (Montreal), A Heartfelt Sadness, what is the connection between depression and heart disease? (Windsor), Aboriginal Health and Cardiovascular and Respiratory Risks (Vancouver) and Oversold on Sodium – How too much salt affects our health? (Toronto).
Media
Media activity is considered an important part of the Institute's public engagement strategy and ICRH has had significant media exposure over the past five years. The Institute is proactive in ensuring that important research findings get exposure in various media in Canada and globally. The scientific director has worked closely with the CIHR communications team, Institute staff and the media to report and discuss research results in the heart, lung and blood domains.
An analysis provided by the communications department at CIHR showed that ICRH has had up to 81 mentions in Canadian media per quarter since 2005. In addition, ICRH ranked from number one to seven of the 13 institutes in terms of number of mentions in the media per quarter.
Health and health system/care impacts
Acute mortality from myocardial infarction and stroke in Canada has steadily declined in the past decade.Footnote 4,Footnote 31 The decline in mortality attributed to treatment advances is about 47% while the remainder is attributed to risk factor identification and intervention.Footnote 4 These major health gains can be credited in large part to the translation of research discoveries into actions for the patient and the public. The improvement in cardiovascular health outcomes has been so consistent over the past few years that by 2011, cardiovascular disease will no longer be the number one killer in Canada. ICRH is currently conducting a return on investment analysis using the payback model; data from this project will be available in late 2010 or early 2011.
While acute mortality from MI has decreased, many cardiovascular and respiratory diseases have now become chronic illnesses. Through research and KT, the incidence of heart failure, which is the number one chronic cardiovascular disease, has begun to plateau.Footnote 31,Footnote 32 The age-adjusted mortality from heart failure has also started to decline, in contrast to a continuous rise seen in earlier years. In addition, the escalating burden of chronic lung disease, especially chronic obstructive pulmonary disease, has begun to decline with respect to mortality and hospitalization.Footnote 5 These trends will translate into many lives saved, much improved quality of life and, eventually, health care cost reductions.
However, with the rising incidence of asthma in children, and increasing obesity, hypertension and lipid abnormalities in people ages 25 to 45, efforts must continue to reduce progression towards end-stage vascular and respiratory complications. ICRH-led initiatives, such as at-risk behavioural interventions and imaging to detect early heart and lung diseases are essential to identify and stem the tide of chronic diseases beginning in early life.
Another example of an ICRH-led initiative that has gained significant momentum and is expected to result in an important impact on health and health care systems is C-CHANGE. One of the barriers to effective development and implementation of guidelines for cardiovascular disease prevention is the complexity and lack of integration of risk factor management. C-CHANGE has harmonized and integrated these complex guidelines and transformed risk management into a patient-centered, coordinated approach to chronic disease prevention.
The C-CHANGE program is supported by the two founding partners: CIHR-ICRH and PHAC. This KT-focused project has now successfully engaged multiple partners, including HSFC, Canadian Hypertension Society, Canadian Diabetes Association and all seven cardiovascular prevention groups and, most importantly, all of the primary care organizations in Canada. The groups have now harmonized and integrated more than 370 recommendations (from more than 1,000 pages of documents) into only 50 essential recommendations. This is accompanied by an implementation strategy and a variety of practice-enabling tools. The recommendations will be introduced in October 2010 with national adoption and tools available for different practice settings. Appropriate indicators have been developed to integrate into the quality improvement strategies in the various provincial jurisdictions. This will maximize their impact.
We believe that C-CHANGE is the first program of its kind in the world, that it will form the foundation of all integrated chronic disease guideline harmonizations in the future, and that it thus represents a major KT innovation.
A manuscript containing the C-CHANGE recommendations has been submitted to the Canadian Medical Association Journal for publication in late 2010.
Transformative impacts
ICRH has played a transformative role in bringing its diverse research communities together to interact, collaborate and create synergies in research and KT. This is evident in such programs as the CVD-Diabetes Initiative, the Gene-Environment Interaction Initiative, where cardiovascular and respiratory teams worked together to characterize population phenotypes and genotypes, and the imaging networks initiative where heart, lung and stroke researchers work together. These are unique collaboration opportunities that could not have happened without ICRH leadership.
ICRH can also be credited for establishing large research networks with significant international links such as the multi-modality imaging network CAIN, which has already produced many high impact publications and competes well on the world stage. Similarly, the Canadian Cohort of Obstructive Lung Disease, Canadian Network and Centre for Trials Internationally and critical care networks are unique national resources that have achieved global impact. Finally, in collaboration with government, the Institute has generated the momentum among the community and stakeholders needed to create three national strategies (the Canadian Heart Health Strategy and Action Plan, the National Lung Framework and the National Sodium Reduction Strategy), all within the past five years. This has been truly a fundamental transformation for the ICRH community. These major initiatives, which promote coordination of research with care and prevention, will continue to make important progress in reducing the burden of heart and lung disease in Canada.
Going Forward
Looking forward to the next decade, ICRH is poised to make further transformations in the health of Canadians. The largest burden of chronic disease is based in heart and lung related areas, yet there has been significant and consistent reduction in mortality from myocardial infarction, stroke, chronic lung disease and asthma. Meanwhile, the number one killer in Canada, cardiorespiratory disease, has been fundamentally altered through research and knowledge translation.
Strategic priorities beyond 2010
CIHR's 2009 Health Research Roadmap, ongoing ICRH programs based on the 2006 ICRH strategic plan and the recently updated ICRH Strategic Plan for 2010–2012, will all serve as a guide for ICRH activities until completion of the 2011 International Review. With the upcoming transition of the Institute's scientific director, the Institute Advisory Board has been mindful of the need for a clear plan to ensure continuity and momentum. The newly updated strategic plan, which was developed based on feedback from ICRH partners and stakeholders through key-informant interviews and surveys of the community, identified specific strategic opportunities to be launched either by the Institute and its partners, alone or in concert with multiple CIHR Institutes.
The following priorities were identified with high potential for leadership by ICRH:
- Environment and cardiorespiratory diseases
- Impact of early identification and intervention on chronic diseases
- Promotion of implementation science – the effect of policy and health system changes related to cardiovascular and respiratory diseases
The priorities recommended for further development by ICRH and its CIHR partners include:
- Early identification of at-risk populations
- Management of chronic illness in the elderly
- Food and cardiorespiratory diseases
- Organ replacement and regeneration
- Quality of care
To achieve "bench to bedside to curbside" innovations, ICRH will take advantage of existing strengths and continue to build new capacity within our research networks, and accelerate the innovation-to-application timeline.
With the confidence earned from past success we expect to see further dramatic reductions in the burden of chronic heart, lung and blood diseases in the next decade. This can be achieved through concerted efforts in earlier disease detection and intervention to prevent complications. In addition, innovative preventive strategies such as redesigning cities and communities, realigning incentives for healthy living and innovative prevention vaccines will together transform disease management and reduce disease burden.
Finally, the potential of regenerative medicine, reprogramming induced pluripotent cells, and innovations in nano-devices and new biomaterials will be realized in the next decade, leading to the development of curative approaches to complement newly implemented disease-management tools. In summary, ICRH will continue to work with its community and partners to move the Institute's mandate forward in a dynamic fashion within the next phase of CIHR's overall mission.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
ICRH specific
| AF–HF | atrial fibrillation – heart failure |
| ARC | average of relative citations |
| C-CHANGE | Canadian Cardiovascular Harmonized National Guideline Endeavour |
| CAIN | Canadian Atherosclerosis Imaging Network |
| CDA | Canadian Diabetes Association |
| CHHS-AP | Canadian Heart Health Strategy and Action Plan |
| CRC | Canada Research Chairs |
| CVD-Diabetes | cardiovascular complications of diabetes |
| DREAM | Diabetes REduction Assessment with ramipril and rosiglitazone Medication |
| HSFC | Heart and Stroke Foundation of Canada |
| IAB | Institute Advisory Board |
| InFACT Network | clinical trial to evaluate novel anti-inflammatory treatments for affected patients |
| KT | knowledge translation |
| MI | myocardial infarction |
| NHLBI | National Heart, Lung and Blood Institute |
| NIH | National Institutes of Health |
| PHAC | Public Health Agency of Canada |
| PPP | public-private partnerships |
| RCC | regional clinical center |
| RELY | Randomized Evaluation of Long-term Anticoagulant Therapy |
| RFA | request for applications |
| ROC | Resuscitation Outcomes Consortium |
| SI | specialization index |
| STIHR | Strategic Training Initiative in Health Research |
| Tekes | Finnish Funding Agency for Technology and Innovation |
| TIMACS | Timing of Intervention in Patients with Acute Coronary Syndromes |
- Date modified: