Internal Assessment for 2011 International Review - CIHR Institute of Gender and Health
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures
- Figure 1: Percentage of total CIHR expenditures related to IGH mandate areas
- Figure 2: Yearly relative change in violence publications, 1997–2008
- Figure 3: Specialization index and average of relative citations for top 10 countries publishing in violence, 2000–2008
Mandate and Context
Mission
The mission of the Institute of Gender and Health (IGH) is to foster research excellence regarding the influence of gender and sex on the health of women and men throughout life, and to apply these research findings to identify and address pressing health challenges. IGH is the world's first and only research funding institute with a specific focus on gender, sex and health – a niche that positions Canada as a global leader in this field. Accounting for gender and sex makes health research more rigorous and more equitably applicable to people's real-world needs. IGH thus plays a unique and instrumental role in enabling the Canadian Institutes of Health Research (CIHR) to fulfill its mandate to promote, assist and undertake "research that meets the highest international scientific standards of excellence and ethics and that pertains to all aspects of health."
A key driver of IGH's work is that every person is gendered and every cell is sexed. Gender refers to the array of socially constructed roles and relationships, traits, attitudes, behaviours, values, relative power and influence that society ascribes to women and men. Gender is often referred to in binary terms (i.e., feminine or masculine); however, there are many locations along the gender continuum. Sex refers to the biological characteristics, such as anatomy (e.g., body size and shape) and physiology (e.g., hormonal activity or organ functioning), that distinguish people identified as female from people identified as male. Many attributes of sex also exist on a continuum. Gender and sex influence health risks, status, behaviours, service utilization and outcomes.
The evolution of Canadian gender, sex and health research
IGH was established in recognition of a need for research to bridge major gaps in the study of the health of women, girls, men and boys. When IGH was created in 2000, a strong cadre of Canadian researchers was studying women's health and Canada was recognized as a world leader in women's health research and policy. Canadian research was rapidly emerging on the biological bases of sex differences in disease occurrence and health outcomes, but the research was neither well-established nor well-funded. Men's health research in Canada was an emergent interest compared with more long-standing work in countries such as the United States, the United Kingdom and Australia. The early years of IGH were dedicated to growing these disparate and unevenly developed research areas into an effective and integrated research community.
In the past decade, IGH has moved from building community to actively driving a cohesive field forward.
Canadian gender, sex, and health research has matured: our acclaimed women's health research community continues to thrive; more researchers are studying the biological bases of sex differences; the once nascent men's health research community has taken root; and, across organizations and disciplines, there is growing recognition of the scientific value of accounting for sex and gender in health research.
We also have seen advances in emerging areas with theoretical and clinical relevance to gender, sex and health research, such as transgender health. Gender and sex considerations are more widely taken up in unprecedented areas of health research and policy, such as drug effectiveness monitoring, care for premature infants and pain research. With a more established field, we are beginning to see that researchers are prioritizing knowledge translation (KT) in their work, a culture that IGH has helped to cultivate. Gender, sex and health research evidence is making a difference as the outcomes detailed in this report make clear. Through its highly engaged relationship with a now robust research community, IGH has been a pivotal agent of these changes.
The Institute is actively strengthening science, catalyzing change and building bridges to improve the health of "every body".
Response to the 2006 CIHR International Review
The 2006 International Review of IGH praised the Institute's achievements during its first five years. The International Review Panel observed that, under the leadership of its inaugural scientific director, Dr. Miriam Stewart, and Institute Advisory Board (IAB), IGH had laid a strong foundation for gender, sex and health research in Canada. IGH was described as a catalyst – a continued strength of the Institute – particularly for building capacity and supporting knowledge creation. The Panel was most impressed with IGH's development of multi-focus, multidisciplinary teams, which they described as "the most successful transdisciplinary program among the institutes." The Panel suggested that the timing was right for IGH to offer larger and longer-term funding opportunities and that consideration should be given to funding junior and mid-career researchers. The Panel further noted that IGH would benefit from increased attention to KT, communications and performance monitoring. In response to this feedback, we implemented significant changes to enhance our institutional capacity in these areas.
Since 2006, we have launched a number of initiatives that have continued to build a strong platform for gender, sex and health research. For example, we funded six Chairs in Gender, Sex and Health (four at mid-career and two at senior levels) and offered a number of larger and longer-term funding opportunities. These included three Centres in Gender, Mental Health and Addictions and five Emerging Teams in Gender, Sex and Health.
To galvanize the Institute's KT and communications portfolios, we instated a dedicated KT staff position and developed and implemented a formal KT strategy. This strategy initiated an important operational shift for the Institute: we embraced communications as a vehicle for knowledge translation, thereby capitalizing on the mutually reinforcing elements of these interlocking portfolios. With the dual aims of strengthening the KT capacity of gender, sex and health researchers and facilitating the translation of gender, sex and health research evidence, IGH has implemented a suite of activities supporting the capture of health research benefits.
To improve performance monitoring we introduced an evaluation plan that supports a culture of evaluation mindedness. Our standard practice is to assess the outcomes of all funded grants and all institute activities, including public events, workshops, training activities, conferences and meetings. We incorporate this feedback into the design of future initiatives. These strategies demonstrate IGH's overarching commitment to achieving organizational excellence.
Our proactive efforts to advance knowledge translation and performance monitoring have enabled IGH to address the evolving needs of its maturing research community.
Institute Priorities
IGH has established a participatory framework for developing institute priorities and the key initiatives for delivering on these priorities. Comprehensive community consultation was integral to the development of IGH's two strategic plans (2000–2008 and 2009–2012) and remains a hallmark of IGH decision making. The consultation strategy employed in developing IGH's second strategic plan was considered a model of best practice and was featured as a case study in CIHR's Citizen Engagement Handbook (2010). Our Institute Advisory Board (IAB), composed of leading researchers from across the field of gender, sex and health, including designates from the voluntary sector and policy and ethics domains, guides the Institute's decision-making process.
IGH is accountable to a broad range of stakeholders, including researchers spanning all four of CIHR's research themes, as well as policy makers, health care providers and representatives of non-governmental organizations. The Institute's consultative strategies build and maintain IGH's credibility and collaboration with the communities it serves, and foster in them a feeling of ownership over the Institute's priorities and activities.
By adopting ground-up decision-making approaches that foster engagement, IGH has positioned itself to be highly responsive to its community and well-equipped to mobilize input for targeting gap areas.
The first IGH strategic plan (2000–2008): Building a community
Under the leadership of Dr. Stewart, the Institute identified five research priorities, each with specific sub-priorities:
- Improving access and equity for vulnerable populations (health equity; access to health services; violence, gender and health)
- Promoting health in the context of chronic conditions (gender, chronic conditions and disabilities; gender and cardiovascular disease)
- Gender and health across the lifespan (healthy child development; healthy aging; work, leisure and health; mental health in a changing society; reproductive and sexual health)
- Promoting positive health behaviours (preventing addictions)
- Gender and the environment (sex, gender and the environment)
The breadth of these priorities gave IGH a foundation upon which to build partnerships and extend its reach across the health research community. This encompassing approach helped diverse constituents find a home within IGH. The priorities were later renewed for 2006–2008 and formed the basis for IGH's strategic investments and activities during that time. The Institute's most significant investments were made in the improving access and equity for vulnerable populations priority and were targeted specifically at the sub-priorities health equity (in terms of reducing health disparities), and violence, gender and health.
The second IGH strategic plan (2009–2012): Leading a field
In 2008, the transition in IGH leadership presented an opportunity to revisit the Institute's priorities in light of advancements in the field. Newly appointed scientific director, Dr. Joy Johnson, launched a second round of national strategic planning consultation. Informed by the consultation feedback, the IAB achieved consensus on six strategic directions. Two of these are overarching capacity-building strategies:
- Advancing methods and measures
- Building partnerships in gender and health
Four are priority topic areas:
- Violence and health: impacts and implications
- Sexual and reproductive health: improved decision making
- Clinical interventions: enhancing effectiveness
- Work and health: research into action
These more focused priorities mark the maturity of IGH and its research community. While IGH remains committed to fostering the integration of gender and sex across the spectrum of health research, the Institute also recognizes its role as a leader in the field of gender, sex and health research. The strategic research directions listed above are areas that the research community identified as significant health issues that would benefit from explicit attention to gender and sex. These areas represent topics not covered by CIHR's slate of institutes and as such underscore the distinctive niche of IGH within CIHR. They also build directly on the initial investments made within the frame of the Institute's earlier, broader priorities.
Key Initiatives
IGH works closely with its community to develop initiatives that address the Institute's priorities. One mechanism through which we solicit input is roundtable meetings with leading researchers and experts from diverse disciplines and sectors. The feedback generated is incorporated into the decision making of our Institute Advisory Board (IAB). An evaluation working group composed of IAB members also provides oversight from the initiative planning stages to final evaluation.
As we develop initiatives, we prioritize partnerships with other CIHR institutes and external partners. We have actively sought out partnerships to grow and leverage our national scientific, social and technical capital in the field, and to foster synergies across funded projects. We recognize that maximizing the potential for the wider integration of gender and sex in health research begins with effective collaboration.
The Institute's engaged approach to initiative development has generated credibility for IGH as an effective convenor and leader.
Of the numerous initiatives launched over 10 years, we highlight three that illustrate IGH's leadership in steering an emergent research community into a fast-growing field. Described below, these initiatives represent areas in which significant funding opportunities were launched and completed, thus allowing evaluation of their outputs and outcomes.
Initiative 1: Capacity development in gender, sex and health
Since its inception, a major cross-cutting initiative of the Institute has been to strengthen Canadian researchers' capacity to address questions in gender, sex and health. Our focus has been not only to bring people into the field, but also to provide them with tools and resources to do the work and demonstrate leadership within the field and beyond.
IGH dedicated earlier efforts to incorporating a new cohort of researchers by focusing on trainee and early-career awards. We developed a number of strategic funding opportunities to stimulate interest among doctoral students, postdoctoral fellows and early-stage researchers in pursuing research careers in gender, sex and health. The Institute invested over $5 million to support 54 training and investigator awards. IGH also invested $8.7 million in CIHR's Strategic Training Initiative in Health Research (STIHR) programs that provided training support for researchers in transdisciplinary areas of study. Since the first STIHR competition in 2001, IGH has contributed to 17 STIHRs that supported 784 trainees.
Having achieved a critical mass of researchers through our earlier capacity development initiatives, we introduced mechanisms to support leadership and recognize excellence among established investigators. In 2007, IGH introduced the Mid- and Senior Career Research Chairs program, which enabled recipients to focus intensively on their programs of research. Six chairs were awarded for a total IGH funding commitment of $4.85 million. All six IGH chairs hold CIHR operating grants and have served on various CIHR peer review panels.
As the momentum for innovation accelerated, we also recognized the need for tailored training that would develop the specialized skill sets needed to move into cutting-edge areas. In 2009, we introduced our annual Summer Institute for graduate students and postdoctoral fellows. Institute curricula blend theoretical and practical considerations related to methods and measures in gender, sex and health research. For the 2010 Summer Institute we developed a toolkit that provided trainees with a suite of resources on conceptualizing and designing health research that accounts for gender and sex.
Initiative 2: Reducing health disparities and promoting equity for vulnerable populations
It is impossible to address health inequities without addressing their gendered dimensions. The overriding importance of gender in producing and addressing health disparities is made clear by the World Health Organization Commission on the Social Determinants of Health's 2008 report, which emphasizes gender as a cross-cutting determinant that interacts with all other underlying factors.Footnote 1 Given that gender is so widely implicated in health disparities, IGH led the development of the Reducing Health Disparities and Promoting Equity for Vulnerable Populations (RHD) initiative. The aim was to develop the multidisciplinary approaches required to design interventions, programs and policies that reduce health inequities in the Canadian population and internationally. This initiative, co-led by the Institute of Population and Public Health, was one of the most partnered initiatives in CIHR's history, involving all of the CIHR institutes, many of its branches and offices and six external partners (Heart and Stroke Foundation of Canada, Public Health Agency of Canada, Health Canada, Social Sciences and Humanities Research Council, National Homelessness Initiative, Citizenship and Immigration Canada).
In total, nearly $15 million was invested in the RHD initiative. Of this, IGH contributed $4.69 million and leveraged an additional $10 million through partnerships with other CIHR institutes and external partners. We began the initiative in 2002 with a series of small pilot grants to build capacity. IGH contributed over $260,000 to fund seven (out of 19) applications; this funding was supplemented with over $330,000 from funding partners. In 2005, with researchers in the field primed to address health disparities, IGH and partners launched the primary component of this initiative: the Reducing Health Disparities – Interdisciplinary Capacity Enhancement Team Grants (RHD teams). With nearly $140,000 from IGH and $30,000 from partners, IGH funded 33 (out of 63) Letters of Intent. At the full application stage, just over $14 million, including all partner contributions and nearly $4.3 million from IGH, were invested in 20 RHD teams (out of 58 applications received). We report on the outcomes of these teams below.
Initiative 3: Violence, gender and health
Violence is a highly gendered phenomenon that significantly affects the lives of individuals, families and communities. Worldwide, about 4,400 people die every day due to the effects of violence and enormous costs are incurred in treating surviving victims.Footnote 2 Since 2001, IGH has supported a range of initiatives focused on violence, gender and health.
The most significant opportunity spearheaded by IGH has been the New Emerging Teams (NETs) program in violence, gender and health. Six teams were funded with a total investment of $5.2 million in 2001 and 2003. The teams were developed to support multidisciplinary research exploring the social, cultural, biological and psychological factors influencing violence, the effects on survivors throughout the lifecycle, and to design prevention and intervention strategies. A unique feature of the violence NETs was the ability to offer funding for new investigators through the team grants.
In 2008, the Centres for Research Development in Gender, Mental Health and Addictions were launched. IGH funded three (out of six) centres for a total investment of $6 million. These three centres each have a core focus on violence. Plans are in place to evaluate the centres at the mid- and end points of their grant tenure.
Outputs and Outcomes
The research and training made possible through the three key initiatives described above have contributed to building Canadian capacity for gender, sex and health research, advancing knowledge and improving health-related decision making. Drawing on data collected through IGH's evaluation of these initiatives and by CIHR's Impact Assessment Unit and Data Analysis Branch, as well as a bibliometric analysis prepared by the Observatoire des Sciences et des Technologies, we highlight some of the outstanding achievements of these initiatives.
The data discussed are robust; however some limitations should be noted. Funding data are based on a keyword search of the CIHR funding database and validated through a subjective process. Projects may have multiple institute affiliations.
Initiative 1: Capacity development in gender, sex and health
Through a variety of significant career and training investments over the past decade, IGH has fostered the development of a highly productive and dynamic research community.
We have been committed to investing in our researchers, and these researchers are demonstrating their enhanced capacity to garner funds and expand the field.
Success in the investigator-driven CIHR Open Operating Grant Program can be used to illustrate the strength of a research community. As shown in Figure 1, CIHR Open Operating Grant expenditures related to IGH mandate areas increased from 2.5% ($6 million) in 2000–2001 to 6.3% ($29.6 million) in 2009–2010. A similar increase is evident for open salary awards and open training awards, where expenditures in IGH mandate areas rose from 1.5% ($382,000) to 7.4% ($1.3 million) and from 1.6% ($480,000) to 6.5% ($3.5 million) between 2000–2001 and 2009–2010, respectively. Expenditures in strategic salary awards in IGH mandate areas increased dramatically from 3% ($119,000) to 16.5% ($1.9 million) in the 10-year period.
Figure 1: Percentage of total CIHR expenditures related to IGH mandate areas
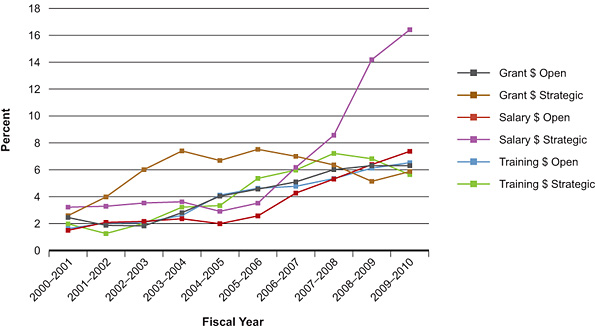
IGH also engages across the spectrum of research. Between 2000–2001 and 2009–2010, IGH-related expenditures increased within each of CIHR's research themes. The greatest increase was in biomedical research, from $1.2 million to $18.3 million (a 15-fold increase), followed by clinical research, from $844,000 to $9.9 million (an 11.8-fold increase), health services research, from $363,000 to $3.4 million (a 9.3-fold increase), and social, cultural, environmental and population health research, from $2 million to $18 million (an 8.8-fold increase).
Not only are gender, sex and health researchers being increasingly funded, they are contributing to new understandings of the relationships between sex, gender and health and moving from description to intervention. A stellar example is Dr. Bill Sheel, an IGH New Investigator Award recipient. In his work on breathing limitations in exercising women, Sheel documented a previously undetected anatomical sex difference: women's airways are up to 22% smaller than men's, even when matched in lung size – meaning that breathing is harder work for women during exercise.Footnote 3 This finding has important implications not only for how sex is accounted for in pulmonary research, but also for tailoring exercise regimes throughout the life course. "We put people into pulmonary rehabilitation and exercise programs and we generally give men and women the exact same 'exercise prescription'. This approach may not be appropriate for a number of reasons; one of them is related to the lungs," explained Sheel.
Another new investigator, Dr. Janice Du Mont, focused her program of research on sexual violence. Her evidence-based recommendations regarding how to support victims of drug-facilitated sexual assault were taken up by Echo, the Ontario government's provincial women's health agency. These recommendations will help the ministry to improve the quality of care offered across Ontario's Sexual Assault and Domestic Violence Treatment Centres.
The New Investigator Awards supported emerging gender, sex and health researchers to launch and intensify programs of research. A shining example of this impact is the success of IGH New Investigator Dr. Ryan Rhodes: "With the teaching load lifted, I have been able to turn my research program into a highly successful, meaningful and prolific enterprise in terms of funding, publications and the training of personnel. It culminated with receiving the 2008 Investigator Award from the North American Society for the Psychology of Sport and Physical Activity. This would not have been possible without the support from IGH." The Institute builds capacity by supporting researchers like Dr. Rhodes to develop top-tier research programs.
In addition to direct capacity enhancement, the New Investigator Awards created spin-off opportunities for up-and-coming trainees. The six new investigators provided training opportunities for close to 30 trainees. It was Dr. Jordan Guenette's undergraduate summer internship with New Investigator Sheel that sparked his interest in sex differences in respiratory exercise physiology. Guenette went on to complete his master's and doctorate with Sheel, meanwhile becoming the first-ever student to win the Canadian Society for Exercise Physiology Graduate Student Award Competition based on a master's level project, and the first student from his department to win a gold medal from the Governor General of Canada. Guenette is now a postdoctoral fellow at Queen's University and told IGH: "My 'success story' is due in large part to the exceptional training and mentorship I received from a CIHR-IGH Investigator. Dr. Sheel has inspired me to pursue a career in academia and to run my own independent research program at a Canadian university where I will focus on sex differences in both health and disease."
As the learning needs of the community have evolved, IGH has responded with new resources and opportunities that are in high demand. There has been strong application pressure for IGH's Summer Institute, which accepts 40 participants per annum (230 applications were received for the 2009 inaugural Summer Institute). Given the limited number of spaces, in 2010 the application process was made more rigorous; still, 150 applications were received. To further expand the accessibility of IGH training, the introductory session of the 2010 Summer Institute was made publicly available live and broadcast online. Approximately 170 people participated from across Canada.
Summer Institute trainees were clear about how IGH enriched their research skills. In follow-up surveys with 2009 participants, trainees impressed upon us how their learning at the Institute influenced their own work. As one participant said, "The Institute enhanced the quality of my research projects because I feel much more comfortable with the concepts of sex and gender and how to apply these concepts methodologically and in analysis of data."
Initiative 2: Reducing health disparities and promoting equity for vulnerable populations
Advancing knowledge
Due to the work of the Reducing Health Disparities (RHD) teams we know more about the nature of health disparities and how best to intervene.
The RHD teams have been exceptionally productive, collectively generating over 400 journal articles, over 200 newspaper/magazine articles and over 80 radio/television presentations, as well as delivering 1,000 presentations at conferences across Canada and internationally. Here we highlight a few of their outstanding contributions to knowledge and how a gender perspective has been central in moving toward evidence-based solutions.
Pinpointing more precisely who is at greatest risk for ill health within vulnerable populations
The team on homelessness, housing and health, led by Dr. Stephen Hwang, is a key example of how teams are generating evidence to promote the development of appropriately targeted interventions. Hwang's team found geographical differences by gender and age in the use of long-stay shelters: older men tended to use these sites in Ottawa and Toronto, whereas in Guelph, younger women were more frequent users. According to Hwang, "From a program planning and policy perspective, this study implies that homelessness prevention strategies would be more efficient if they were specifically aimed at [population] clusters."
Using a gender lens to generate new insights about the nature of health disparities
A standout example of the advances in knowledge made possible through the RHD initiative is the Stigma and Resilience among Vulnerable Youth Consortium led by Dr. Elizabeth Saewyc.Footnote 4 This team completed the largest study of sexually exploited youth in North America to date. Using a youth- and community-engaged approach with a gender-based analysis, the knowledge generated exploded common stereotypes: street-involved boys were just as likely to be sexually exploited as girls, both at age 13, on average; and it was not just men who exploited youth: 79% of sexually exploited boys reported having been exploited by women (54% of them solely by women). Such knowledge informs outreach programs targeting high-risk youth.
Shedding new light on the role of gender in producing health disparities
The Cardiovascular Secondary Prevention for Vulnerable Populations team, led by Dr. Sherry Grace, is a prime example. This team documented that Canadian women reported significantly greater barriers to accessing cardiac rehabilitation services than men.Footnote 5 "Our research has shown that we can equitably refer men and women to cardiac rehab, but that women have specific barriers to enrolment that must be addressed in future work," explained Grace. This finding led the team to secure funding for a randomized controlled trial of women-only cardiac rehabilitation, the first of its kind in Canada. The team also developed a gender-sensitive scale for assessing barriers to cardiac rehabilitation that is freely available to health practitioners online.
Informing decision making
Knowledge users are taking up the new knowledge produced by the RHD teams.
IGH developed this initiative with knowledge users in mind, and the teams were extremely successful in establishing meaningful partnerships and collaborative relationships with policy makers and practitioners to inform policy and practice changes.
Working with government agencies to make change
Dr. Jean Shoveller's Youth Sexual Health Team is a shining example of an RHD team adept at working with agencies to make change. This team identified vulnerable groups that were not accessing sexually transmitted infection testing, including youth and men who have sex with men. The team's work highlighted how gender-based factors, such as young boys and men having significant misinformation about sexually transmitted infection testing processes, created barriers to access. To address this, the team partnered with the British Columbia Centre for Disease Control to develop and offer online facilitated testing for sexually transmitted infections. Together, they are launching a new program of research related to the implementation and evaluation of online assessment and testing (including computer-generated lab requisitions and self-swabbing) for sexually transmitted infections.
Developing innovative tools to support informed decision making
Innovative modes of dissemination developed by the RHD teams have increased the accessibility and usability of their research evidence. Dr. Jude Kornelsen's team, Appropriate Access to Maternity Services for Rural Women, is a model of effective knowledge translation. The team developed the Rural Birth Index, an evidence-based tool for assessing maternal health care needs in rural areas.Footnote 6Using the Rural Birth Index, the team helped to inform the process for prioritizing rural health services in British Columbia. "Since its development in 2007 and publication in 2009, the Rural Birth Index has been used to strengthen advocacy for vulnerable populations by quantifying a community's need," explained Kornelsen.
Creating hubs for specialized expertise
By supporting knowledge "economies of scale", the team grants enabled RHD teams to capitalize on their collective expertise and come to be recognized as sources of credible information. A major success story is the case of Dr. Danielle Julien's team, Sexual Vulnerability and Resilience among Sexual Minorities in Canada. Team members, professors Bill Ryan and Line Chamberland, were appointed to a working group on homophobia convened by Quebec's Ministry of Justice in 2005. Additional team members also provided expert testimony during the working group's consultation process. Published in March 2007, the report made firm recommendations to the Ministry of Justice for crucial policy changes to support equality for sexual minorities.Footnote 7 These included the need to support research to fill gaps in knowledge about sexual minority women relative to sexual minority men. It also advocated for targeted public services, including health. Based on this report, the Quebec government adopted an official policy against homophobia in December 2009 and mandated a multi-ministerial committee to define an implementation plan forthcoming in December 2010. Research by Julien's team was cited extensively in the report and the policy.Footnote 8
Capacity building
The RHD initiative created a new cohort of promising researchers and enabled established researchers to intensify their programs of research in health disparities from a gender perspective.
Collectively, the RHD teams leveraged more than $40 million in additional funding, a significant portion of which was devoted to training support for graduate students and postdoctoral fellows recruited to work with the teams. The sheer number of emerging researchers brought onboard is a strong indicator of the capacity built through the RHD teams: more than 100 master's students, 80 doctoral students, 30 postdoctoral fellows, 35 clinical fellows and 40 early-career investigators.
An example of the teams' commitment to capacity building is the trainee-centred approach adopted by Dr. Jude Kornelsen's team on rural maternity care. With the aim of providing opportunities for future rural health researchers and instilling interest and skills in rural health services, the team supported 27 students over five years through various work-study programs. The team also supported additional doctoral positions to investigate rural maternity care and made a point to hire students from across disciplines to assist with their projects.
The RHD grants were career-changers for established and newer researchers. The grants afforded opportunities to expand into cutting-edge areas, intensify programs of research and foster the involvement of knowledge users and researchers at various career stages. Kornelsen explained, "As opposed to gathering data to answer one question, we are able to engage in a series of questions, the answers to which provide a richer understanding of rural maternity care than if the projects were done in isolation. As I have seen the benefits of this engaged approach to research, it has informed the way in which I will take up doing research for the rest of my career."
For Dr. Danielle Julien and her sexual vulnerability and resilience team, the RHD team grant enabled the group "literally to get the research off the ground" and cement their expertise in health disparities among sexual minorities. Julien shared an example of how her team had transformed the context for this work: "A new researcher once told me about how she felt isolated, alone, and without resources in pursuit of research on sexual minorities and health. Recently she said to me: 'I am with a growing number of other researchers in this area. I feel their support and concern. They enable me to share the confidence in the work we are doing.' Together we have built a truly worthwhile research environment that is the basis for advancing research on these vulnerable groups." This example points to the important role that teams can play in creating the type of linked-in community that supports capacity.
Initiative 3: Violence, gender and health
Advancing knowledge
The work of the New Emerging Teams (NETs) in violence, gender and health has enhanced understandings of the outcomes and costs to society of violence and introduced new ways to intervene.
The six NETs were exceptionally productive, generating more than 110 journal articles and more than 450 conference presentations in Canada and abroad. The teams' activities also garnered significant media attention, including over 30 newspaper/magazine articles and 20 radio/TV presentations.
Given the focused nature of this initiative, a bibliometric analysis of publications in violence was undertaken to gain a sense of Canada's relative international standing in this research area. Publications on violence were identified through medical subject heading searches completed by the Observatoire des Sciences et des Technologies. Databases searched may not cover all publications in this area. The data for average of relative citations (ARC) – the average number of citations attributed to papers in violence and health over a two-year period following the publication year – is incomplete for 2008. Countries were ranked based on total number of publications from 1997–2008.
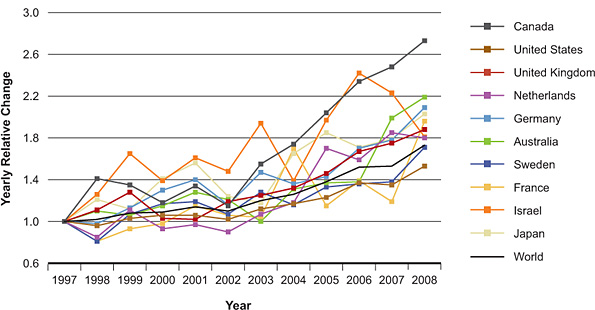
The number of violence and health publications in the world per annum grew from 2,265 in 1997 to 3,917 in 2008. As Figure 2 demonstrates, among the 10 top-publishing countries in the field, Canadian research in violence and health has had the largest relative change since 1997. Having risen steadily since 2002, Canada emerged in 2008 as the country with the highest relative growth in violence and health publications, with an increase from 110 (1997) to 300 (2008) publications. Given the number of publications (115) by IGH-funded NETs, these researchers contribute substantially to the growth in this area.
Figure 2: Yearly relative change in violence publications, 1997–2008
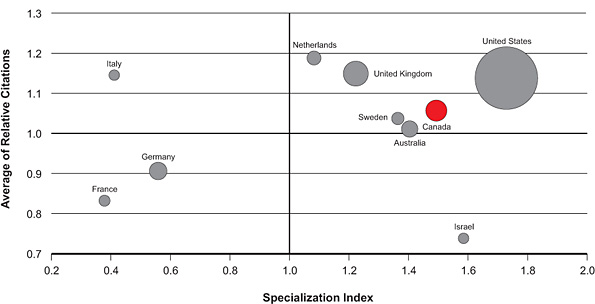
Other bibliometric indices suggest that Canada is a leader in research on violence and health. In Figure 3, the circle size corresponds to the number of publications produced in this research area between 2000 and 2008. Canada has produced 1,818 publications in violence and health, ranking third among the top 10 countries. Canada is currently ranked fifth (1.1) for ARC in the area of violence and health. The specialization index (SI) represents the relative intensity of publications by country in a particular area relative to the intensity of the world. Canada's SI for publications in the area of violence and health is ranked third after the United States and Israel. In sum, Canadian publications in the field are more specialized than, and cited as frequently as, the world average. Below are some key examples of how IGH NET investigators are advancing this body of knowledge.
Figure 3: Specialization index and average of relative citations for top 10 countries publishing in violence, 2000–2008
Identifying new causal pathways and types of violence
The Health Impacts across the Lifespan team, led by Dr. Harriet MacMillan, is a landmark example of the new knowledge contributed by the Canadian contingent. The IGH violence team grant served as a springboard for work in the areas of child maltreatment, intimate partner violence and elder abuse. In relation to this first area, the team uncovered new links between exposure to violence in childhood and adult impairment including substance abuse and mental health problems. The team's foundational work in intimate partner violence led directly to the development of the McMaster Violence Against Women Research Program, funded by the Ontario Ministry of Health and Long-Term Care–Ontario Women's Health Council, which examined the health care response to intimate partner violence, especially the effectiveness of screening women for abuse in health care settings.Footnote 9 The team identified previously unreported forms of elder abuse, including physical and sexual victimization, financial abuse and abuse by those within the medical system. Their findings underscored that gender plays an important role in elder abuse experiences.
Expanding understanding of the gendered health effects of violence on particular at-risk groups
A striking example in this area is Dr. Christine Wekerle's Maltreatment and Adolescent Pathways (MAP) study. MAP followed a group of adolescents in government child protective services who were maltreated in childhood to understand their experiences of violence over time. This type of longitudinal work – obtaining baseline measures on child maltreatment experiences, and then repeated measures of adolescent dating violence, unsafe sexual activities and self-inflicted violence – is a world first. MAP generated new knowledge about how recovery from and coping with child abuse and neglect differs for boys and girls.Footnote 10
Pioneering new methods and measures to capture the gendered health effects of violence
Longitudinal research on intimate partner violence is extremely rare, in part due to the methodological challenges associated with accessing and retaining participants. In one of the few longitudinal studies in the world on intimate partner violence, Dr. Marilyn Ford-Gilboe's team documented the existence of long-term mental and physical health problems for abused women, even after having separated from their abusive partners. In addressing these multiple and often chronic health consequences, abused women accessed health and social services at higher than average rates. Using a novel methodology, the team estimated partial public and private costs attributable to intimate partner violence to be more than $13,000 per woman per year, or a national cost of $6.9 billion annually.Footnote 11 The team has designed a complex primary health care intervention being piloted in New Brunswick and Ontario that is tailored to the health and social needs of women who have separated from an abusive partner.
Extending understandings of the links between violence, gender and health
One important contribution in this area is the work of Dr. Debra Pepler's Preventing Violence in the Lives of Girls and Women team. This team sought to understand why aggressive girls have more mental and physical health problems than do non-aggressive girls. They found that important contextual factors including growing up in a chaotic household, being unable to follow a routine and having disrupted relationships with parents and caregivers all contribute to the poor health outcomes experienced by aggressive girls.Footnote 12
It is clear from the bibliometric data and these examples of work by our violence NETs that Canadian researchers, supported by IGH, are driving the field of gender, sex and health in new directions of international significance.
Informing decision making
Extending the culture of partnerships fostered by IGH, the violence, gender and health teams successfully collaborated with decision makers and mobilized evidence to inform health decision making.
Developing strong partnerships to move evidence into action
Dr. Debra Pepler's team on violence, girls and women is a stellar example of how teams have established effective partnerships to move evidence into action. This group developed the Promoting Relationships and Eliminating Violence Network (PREVNet), which brings together 65 Canadian researchers and their students with 51 national youth-serving organizations to develop, exchange and mobilize knowledge. The Boys and Girls Club of Canada is one of the many strong partners with whom they have developed training and strategies to address social-aggressive behaviour based on PREVnet evidence and approaches.
Collaborating to scale up evidence-informed solutions
Dr. Marlene Moretti's team on aggressive and violent girls is an example of how teams have collaborated to expand the reach of their interventions. This team worked with the British Columbia Ministry of Children and Family Development to roll out an intervention for adolescents with aggressive and antisocial behaviour. Standardized training and supervision were provided to practitioners who delivered the program in 17 communities serving 309 parents and their families. Results from this program showed significant pre- to post-treatment reductions in teen problem behaviour, enhanced teen social functioning and improvements in teens' capacity to manage difficult emotions.Footnote 13 By effectively connecting with the ministry, Moretti's group was able to translate its research into a successful and widely-available ministry program to support healthful development in children and teens. This shows how IGH teams are not only informing decision making, but also developing the enduring partnerships in the policy arena that are necessary to move into large-scale interventions.
Modeling successful knowledge translation practices
IGH teams in violence are modeling for others how to undertake knowledge translation and develop interventions that take gender into account. Members of three violence NETs (Drs. MacMillan, Ford-Gilboe and Wekerle) convened the "TriNET" Family Violence Knowledge Exchange Forum in Toronto (January 2009). This meeting brought together health and social service policy makers, planners, frontline practitioners and advocates with researchers from a variety of jurisdictions concerned with child maltreatment and violence against women. The forum established important relationships that are now in place for the teams' intervention programs. The lessons learned from TriNET were shared in a CIHR knowledge translation casebook (2010). Another example is Breaking the Cycle – a child maltreatment prevention program for substance-using mothers and their young children – developed by Dr. Debra Pepler's team. This was recognized as a model program by the United Nations Office on Drugs and Crime.Footnote 14
Capacity building
One of the major successes of the New Emerging Teams in violence, gender and health was their capacity to attract trainees to their research and ultimately to pursue careers in the field.
The teams were extremely successful in bringing new students and early-career investigators into the fold, collectively recruiting 24 master's students, 23 doctoral students, and 21 postdoctoral fellows.
Through the violence teams, new researchers were able to develop field-specific research skills, expand their collaborative networks, gain exposure to large empirical projects and partake in policy discussions. Dr. Christine Wekerle's team facilitated leadership roles for trainees by co-authoring papers, presentations and grants focused on violence. Working closely with a large team also provided unique opportunities for trainees that were not available through traditional learning channels. As another team leader, Dr. Debra Pepler, explained, "Formal training for most emerging researchers these days does not give the proper skills needed to work with frontline organizations. This kind of work requires a different understanding; it requires a different pace and learning in both directions. We had the opportunity to provide this training by working with our partners." These learning experiences significantly prepared up-and-coming trainees to work collaboratively in the field and to succeed.
The team grants program funded new investigators, affording them the support, time and infrastructure to obtain further funding and launch their own programs of research. Wekerle stressed how the team environment enabled new researchers to develop dedicated careers in violence, gender and health by providing "a substantial support and safety net to take on the risks of moving into novel areas." By igniting and fuelling original research by new investigators, the teams significantly enhanced Canadian capacity for leadership and innovation in the field of violence, gender and health.
Other indicators of growing capacity include how the teams leveraged new funds and opportunities. Dr. Harriet MacMillan's team, for example, received funds for one of the three IGH Centres in Gender, Mental Health and Addictions. According to MacMillan it was the valuable relationships developed through the violence team grant that enabled her to identify 16 partners in her centre grant application, including the World Health Organization, the Child Welfare League of Canada, the Mental Health Commission of Canada, Health Canada and the Public Health Agency of Canada, among others. Likewise, the significant contributions that Dr. Marlene Moretti made to the field of violence and health through her team grant positioned her to compete successfully for a prestigious IGH Research Chair in Gender, Sex and Health. These achievements highlight the productivity and level of excellence supported through the violence NETs.
Transformative effects of the Institute
IGH has transformed the research landscape: Canadian capacity for gender, sex and health research stands strong; we know more about the nature of health and illness; and positive changes in practice and policy are taking place.
A thriving Canadian gender, sex and health community
Through strategic investments, IGH has created a productive research environment for gender, sex and health researchers. Canada is at the cutting-edge of this field, due in no small part to the targeted investments of IGH. We have a strong and flourishing community of researchers who are studying health issues across the spectrum of health research. The next generation of health researchers is better equipped to consider the influences of sex and gender on critical health outcomes. The overwhelming response to the call for abstracts for the first-ever national conference on gender, sex and health (November 2010), organized by IGH, is testimony to the thriving state of the science in Canada. New understandings of how gender and sex affect health and disease are leading to improved interventions and policies.
An emerging culture of knowledge translation
The field of gender, sex and health has been largely focused on describing gender and sex differences, and is now beginning to address the inequities that arise from them. We are cultivating a culture of knowledge translation (KT) and intervention for gender, sex and health research in Canada. As the role of IGH has evolved from building a community to leading a field, so too has the focus of the field shifted from describing phenomena to building on those understandings to derive appropriate solutions. As illustrated, IGH-funded research is making a difference in the health of Canadians. Research priorities identified at our roundtable consultations consistently reveal a strong focus on KT, a promising indication that KT is gaining prominence in the field.
IGH has laid the groundwork for this shift through several mechanisms. The strategic priorities of our latest strategic plan (2009–2012) are infused with KT commitments: improving decision making, moving research into action and enhancing effectiveness. KT-specific objectives and requirements are now consistently embedded in our funding architecture, supporting a research context that favours KT. We have strategically invested in funding opportunities that expand the possibilities for KT in the field. In partnership with the CIHR KT Branch, IGH funded seven knowledge synthesis grants from 2006 to 2009 focused on topics in gender, sex and health. IGH's recent investments in Emerging Teams in Gender, Sex and Health as well as the three Centres for Research Development in Gender, Mental Health and Addictions support the development of the multidisciplinary, cross-theme and inter-sectoral infrastructure requisite for KT. The centres are specifically mandated to develop interventions and create program and policy improvements.
Positioning the Institute as proactive with regards to KT has enabled IGH to drive its solutions-focused mandate forward, advance the KT directions in CIHR's strategic plan and continue to meet the evolving needs of a maturing research community.
Mainstreaming gender, sex and health
IGH is working to integrate gender and sex considerations into all levels of health research, policy and practice – a transformation also known as mainstreaming. We are making headway. Where once the role of gender and sex in health policy and practice was questioned, researchers are now recognizing that pre-clinical studies cannot be confined to male animals only, that it cannot be assumed that a drug or device has similar functions for males and females or that men and women access care in the same way.
Partnerships are an avenue through which the Institute has made inroads into mainstreaming. We have drawn on our position as a cross-cutting institute to promote the inclusion of gender and sex considerations in the work of other institutes and organizations. We do this by providing the tools necessary to conduct gender- and sex-based analyses (i.e., methods and measures) and by offering direct research support through partnering on funding opportunities. In developing our current strategic plan, we identified partnership building as one of our two overarching capacity-building strategies.
In the public realm, IGH has expanded the potential for uptake and the scope of engagement with gender, sex and health research. It is now our standard practice to couple all Institute Advisory Board (IAB) meetings with public engagement events, in addition to our ongoing outreach programming. Our Café Scientifiques, a series of public discussion sessions on research, have been met with high demand. One of our Café Scientifiques, called The Strong, Silent Type: Men's Mental Health and Illness (Vancouver, June 2008), was so well attended and received such significant media coverage, including radio spots on CBC Radio One, that we repeated the Café in another city (Ottawa, March 2009). Gender and health matter to Canadians.
We have shifted policy within CIHR. In 2006–2007, we produced and disseminated "Gender and Sex-Based Analysis in Health Research: A Guide for CIHR Researchers and Reviewers" to all 52 CIHR peer review committees and to federal and provincial funding agencies. Because of the dedicated efforts of IGH, these principles were incorporated into CIHR policy documents and integrated into guidelines for strategic and open competitions. CIHR will now be instating two new mandatory questions in CIHR's standard grant application form: are sex (biological) considerations taken into account in this study? (i.e., are males and females included, or relevant sex-based biomarkers considered?); and are gender (sociocultural) considerations taken into account in this study?
IGH played a key role in the revision of the Sex and Gender-Based Analysis Policy of the Government of Canada's Health Portfolio, which reads: "It is the policy of the Government of Canada's Health Portfolio to use sex and gender-based analysis to develop, implement and evaluate the Health Portfolio's research, programs and policies to address the different needs of men and women, boys and girls." CIHR is a signatory on this policy and IGH is now helping to develop a CIHR action strategy to ensure effective implementation.
Although these successes cannot be attributed solely to the work of IGH, the very existence of IGH has been a beacon for transformative change. We have made it a point to embrace and expand this into a catalytic role.
Going Forward
In building on the momentum of the past decade in gender, sex and health research in Canada, we are eager to pursue directions that will continue to advance the field. These directions encompass both leveraging the strengths of investments made and defining new target areas to push the field forward, as well as further developing the way that IGH serves an expanding research community.
Emerging issues
As we move into the second decade of IGH's work, several issues will require attention. We must continue to strike a balance between investing in the priority areas of IGH and partnering with others on their priorities by bringing sex and gender concerns to the strategic work of the other institutes.
We foresee a number of challenges related to ethics that will require our attention. For example, it is clear that the study of sex and gender differences can at times have the unintended consequence of making unfounded generalizations about men and women or particular types of men and women. We need to continue to reflect critically on how sex and gender are applied in research. IGH has begun to actively integrate ethics into its research priority decision-making processes, research training and research policy involvement. Ethics researchers were purposely included in IGH's roundtables on violence and cardiovascular disease, and their input informed the development of subsequent funding opportunities.
IGH has been successful in supporting research across the continuum, from the bench to the community. As we move forward we need to continue to develop opportunities and initiatives that will engage these diverse constituents and encourage them to work together. Given our limited funding envelope we will need to continue to find creative ways to leverage our research funds.
Another emerging issue is related to the need for increasingly nuanced approaches to the study of gender and health. Gender is not a monolithic category; it is a social location that interacts and intersects with numerous other social locations including age, race/ethnicity, and socioeconomic status, to name a few. An emerging body of work is addressing these intersections. As the Institute of Gender and Health, we need to continue to advance our understandings of these interrelationships.
Developing new knowledge
With the phased approach we have taken to implementing our most recent strategic plan, we have yet to develop funding initiatives in the area of work and health. Work roles and workplaces involving paid and unpaid work are shaped by gender and sex, making this area a niche interest. In the coming year, we plan to engage the work and health research community – a community whose focus does not traditionally align with the mandates of any of the 13 CIHR institutes – to explore areas where research funding is needed.
With respect to our priority on sexual and reproductive health, sexual health has been the focus of several Reducing Health Disparities teams and we have undertaken some initial work through partnerships. We now need to determine the gaps that will inform our future strategic work in this priority direction.
Another area we aim to target is health services. Among the four CIHR themes, health services research has received the least funding from the CIHR Open Operating Grant Program in IGH mandate areas. There is emerging evidence that the differential access and care experienced in the Canadian health system is highly gendered. Health systems need to be responsive to the needs of both men and women, and we look forward to addressing this gap though partnerships with the Institute of Health Services and Policy Research and the wider health services research community.
Continuing to strengthen the research community
In the early phases of IGH, most successful applications for strategic funding opportunities focused on women's health issues. We realized that if we were to be an institute of gender and health, we needed to strengthen the area of boys' and men's health. Having recently launched initiatives focused specifically on boys' and men's health, we will continue to ensure that our forthcoming initiatives explicitly encourage studies to support growth in this area.
We are continuing to enhance the infrastructure needed to propel Canadian gender, sex and health research to new levels. In addition to creating new opportunities, we are forging synergies and strengthening networks among the established chairs, centres and teams to share information and to collaborate. We host teleconferences so that awardees can apprise one another of their initiatives and discuss potential collaborations. We are actively engaging these leaders in discussions about the evaluation of their work. We make a point of highlighting their work on our website and in newsletters. We look forward to expanding on these activities to further strengthen the platform for gender, sex and health research in Canada.
Advancing the science of gender, sex and health
Methods and measures are the approaches, procedures and conventions that researchers use to collect and analyze data reliably and credibly to address research questions. Many studies of gender, sex and health have tended to compare women and men on various health indicators. While this is an important starting point for noting similarities and differences between the sexes, it does not illuminate the underlying mechanisms behind these differences. More sophisticated approaches are required to uncover the nature of these relationships.
To address this health research gap, IGH identified advancing methods and measures for research on gender, sex and health as a priority, and launched an initial Catalyst Grant funding opportunity in 2009. In going forward we will expand our work on this priority. We are developing training opportunities and resources that make evident the innovative ways in which sex and gender have been integrated into health research. We have developed and are refining guides and tools for peer reviewers to help them raise key questions about sex and gender in the peer review process.
Delivering on Health Research Roadmap
To be effective as an organization, all CIHR institutes need to collaborate to achieve a common mission. IGH is playing an important role in helping CIHR deliver on its strategic plan, Health Research Roadmap. We are increasingly aligning our activities with Roadmap. Because gender and sex is "every body's" business, we see strong integration of IGH's interests with all priorities in Roadmap. For example, our strategic priority related to enhancing the effectiveness of clinical interventions aligns strongly with the Roadmap priority related to enhancing patient-oriented care and we will be launching an initiative related to cardiovascular disease in 2010–2011. IGH's strategy on knowledge translation links directly to and helps deliver on the Roadmap directive to accelerate the capture of the health and economic benefits of health research. Reinforcing the directions and delivering on the goals of Roadmap through our Institute's activities is an ongoing priority.
Lessons learned
Lessons learned from the work of IGH over the past decide form the basis of our way forward as we advance the mission of the Institute. Key among these is recognition that the research community must be engaged in the development of research initiatives to identify meaningful priorities and to craft stronger research funding opportunities. A related lesson is the importance of designing funding opportunities that will encourage researchers to draw decision makers and community members into their research. It is these partnerships that will help to ensure that research findings are moved into practice.
A third lesson is that researchers, clinicians and policy makers are open to the idea that sex and gender matter to health research, policy and practice. Sometimes it just takes one simple question – "Do you know the sex of your cell line?" – to spark an awareness of these issues that grows into a way of doing research. As an institute known for its leadership, IGH will continue to foreground questions of gender and sex with our colleagues and research partners, and wherever the opportunity presents itself. Going forward we will address emerging issues, develop new knowledge, strengthen the research community and advance science by keeping gender and sex at the centre of health research.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
IGH specific
| ARC | average of relative citations |
| IAB | Institute Advisory Board |
| KT | knowledge translation |
| MAP | Maltreatment and Adolescent Pathways |
| NET | New Emerging Team |
| PREVNet | Promoting Relationships and Eliminating Violence Network |
| RHD | Reducing Health Disparities |
| SI | specialization index |
| STIHR | Strategic Training Initiative in Health Research |
| TriNET | a meeting of three NET teams |
- Date modified: