Internal Assessment for 2011 International Review - CIHR Institute of Population and Public Health
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Initiative 1: Demonstrating scientific leadership for public health revitalization in Canada
- Initiative 2: Catalyzing the shift from describing determinants of health to an examination of pathways to health equity
- Initiative 3: Building the field of population health intervention research
- Cross-initiative public health system impact and transformative effects
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures
- Figure 1: Percentage of total CIHR expenditures related to theme 4 research since 2000
- Figure 2: ARC and SI for top 10 Countries publishing in health status
disparities, 2000–2008 - Figure 3: Health disparities/equity/inequalities-related theme 4 expenditures and number of grants by fiscal year
- Figure 4: Population health intervention research-related theme 4 expenditures and number of grants by fiscal year
Mandate and Context
Leading Canadian population health scientists have contributed to our understanding of why some people are healthy and others not. "Whatever is 'going around', people in lower social positions tend to get more of it and die earlier – even after adjustments for the effects of specific individual or environmental hazards."Footnote 1 Advances in population and public health science and its direct translation into programs and policies are critical to achieving further improvements in the health of populations and to reducing health inequities.
The Institute of Population and Public Health (IPPH) was established in 2000 with an integrative mandate: to support research into the complex biological, social, cultural and environmental interactions that determine the health of individuals, communities and global populations; and to apply knowledge to improve the health of individuals and populations through strategic partnerships with population and public health (PPH) stakeholders and innovative research funding programs. The IPPH mission is to improve the health of populations and promote health equity in Canada and globally by supporting research and encouraging its application to policies, programs and practices in public health and other sectors.
IPPH plays a dual role in the Canadian Institutes of Health Research (CIHR). It works externally with public health and population health researchers and partners and internally to enable CIHR portfolios and institutes to meet their theme 4 mandate under the CIHR Act (i.e., to support research focused on the health of populations, societal and cultural dimensions of health and environmental influences on health).
The Institute's ambit brings together the connected fields of population and public health. These fields have strong roots in a range of health and social disciplines, including epidemiology, biology, psychology and sociology, to name a few. Canada's scientists have established important conceptual foundations for population health science.Footnote 2 Population health involves a transdisciplinary approach to understanding the determinants of human health at individual and community levels, across societies and over the life course. In particular, it examines the interaction of people's physical and social environments with their biological and genetic predispositions. RoseFootnote 3 hypothesized that larger improvements in population health might be achieved through interventions aimed at social, cultural and environmental determinants of health than through initiatives targeting individual patients and their families. This proposition is not only relevant to IPPH but also underpins CIHR's fourth theme of research.
The complementary focus of IPPH is public health – the health sector primarily concerned with addressing the determinants of health through organized societal efforts directed at the health of whole populations rather than individuals.Footnote 4 Most public health services in Canada are under provincial or territorial jurisdiction with some exceptions such as First Nations and Inuit health services and Canada's Quarantine Act. Public health garners only 6 to 7% of all health system funding in Canada.Footnote 5
The PPH research environment in Canada was not well developed when IPPH was created. Training opportunities were limited, there were no schools of public health, federal funding for population health research had disappeared with the closure of the National Health Research and Development Program in 1999 and there was no national agency for public health. As such, dedicated investments were needed to build PPH research capacity. The severe acute respiratory syndrome (SARS) outbreak in 2002 and the federal government's post-SARS reportFootnote 6 highlighted major gaps in Canada's public health capacity, both in front-line service delivery and in the generation and use of scientific evidence.
Many changes have taken place in Canada's PPH landscape since CIHR's first international review, including:
- The expansion of graduate education programs (growth to 13 Master's of Public Health programs and five Schools of Public Health in existence in Canada)
- The establishment of the Public Health Agency of Canada (PHAC) and six National Collaborating Centres for Public Health (NCC) focused on knowledge synthesis, translation and exchange for public health policies and programs
- The creation of a provincial public health agency in Ontario that complements existing agencies in Quebec and British Columbia
- The introduction of major provincial public health reforms in several provinces, including legislation for core public health standards
These recent structural changes have strengthened training, infrastructure and leadership opportunities for PPH research and knowledge translation (KT) in Canada. IPPH, with partners, has capitalized on these changes to advance its strategic priorities while building capacity for PPH research. Despite considerable achievements over the past 10 years, the Institute's job is not finished. This report describes how IPPH has maximized its impact through strategic investments and helped transform PPH research in Canada. It also discusses areas for further development and IPPH priorities going forward.
Institute Priorities
To inform the first and second strategic plans, IPPH undertook extensive, pan-Canadian consultations within and beyond the population and public health (PPH) research community and sought direction from its Institute Advisory Board (IAB).
Launched under the Institute's first Scientific Director, Dr. John Frank, IPPH's inaugural strategic plan (2002–2007), Mapping and Tapping the Wellsprings of Health addressed five research niches and gaps: building capacity for relevant cutting-edge PPH research and its use by decision makers; understanding and addressing the impacts of physical and social environments on health; characterizing and reducing health disparities; understanding the environmental and genetic determinants of disease in human populations; and supporting global health research.
The Institute's early recognition of global health research as a priority catalyzed this field in Canada by advancing understanding of the ecological, technological, economic, political and socio-cultural forces which shape health. The IPPH leadership in establishing and implementing the Global Health Research Initiative (GHRI), contributed directly to CIHR's mandate to advance research that will improve the health of Canadians and the global community.
Based on a review of investments and the advice of the IAB, these strategic priorities continued to guide the Institute's directions until the second strategic plan was developed under the leadership of the current Scientific Director, Dr. Nancy Edwards, who began her term in July 2008. The 2009–2014 strategic plan, Health Equity Matters, builds on IPPH achievements and Canada's growing capacity in PPH and responds to gaps identified by stakeholders and recommendations of the first international review. This plan is also in line with landmark reports by the World Health Organization's (WHO) Commission on Social Determinants of Health, Canada's Chief Public Health Officer and the Senate Subcommittee on Population Health. The plan also aligns with CIHR's Roadmap. Strategic priorities include: understanding pathways to health equity; population health intervention research; implementation systems for population health interventions in public health and other sectors; and theoretical and methodological innovations in PPH research, knowledge synthesis and knowledge translation.
Several key changes are noteworthy in the current IPPH strategic plan. While the first plan focused on understanding the physical and social determinants of health and explicitly targeted global health research, the current plan emphasizes the advancement of knowledge about population health interventions and their impacts on health and health equity. It also underscores implementation systems for the governance and scaling-up required to deliver these interventions in health and other sectors. IPPH remains a key champion for global health research within and beyond CIHR.
Response to 2006 International Review
As observed in the first international review, IPPH was starting only from the basic building blocks for an Institute, while many other institutes benefited from the long-term support of previous Medical Research Council of Canada collaborations. The review recommended that IPPH sustain and expand its partnerships, KT, communications and stakeholder engagement activities. It also encouraged the Institute to place more emphasis on ethics, research and funding mechanisms for intervention, mid-career salary support and on internal performance measurement and evaluation. The review acknowledged the dual role of IPPH as an Institute and in promoting theme 4 research and suggested clarifying who is responsible for funding this research within CIHR. Over the last five years, as demonstrated in this report, IPPH has bolstered its investments in KT and communications, developed a population health ethics initiative, launched a mid-career salary support program and extended partnerships with key national and provincial organizations.
Key Initiatives
Three key strategic initiatives best illustrate the Institute's role in successfully catalyzing population and public health (PPH) research of national and global importance. While the context, strategy and major achievements for each initiative are described in this section, the Outputs and Outcomes section details IPPH-led and co-led funding competitions that support key indicators. These initiatives demonstrate the function of the Institute in garnering strong application pressure, leveraging partner funds and responding to the needs and niche strengths of Canada's PPH scientists while addressing research questions of central relevance to decision makers.
Initiative 1: Demonstrating scientific leadership for public health revitalization in Canada
IPPH identified critical gaps in PPH research environments and front-line capacity during its 2001 consultations and these system-level deficiencies were further exposed during the severe acute respiratory syndrome (SARS) crisis. Since that time, the public health landscape in Canada has changed considerably and the Institute has adapted to this dynamic context accordingly. As a result of IPPH's demonstrated leadership, the renewal and revitalization of the public health system and PPH research in Canada has occurred in lockstep. Specifically, IPPH has established strong foundations for graduate training, salary support for exceptional mid-career scientists and enduring PPH research environments through the Centres for Research Development program. The Institute has also initiated deliberate collaborations for leading-edge research and its translation into public health programs and policies by current and future generations of scientists and decision makers. For example, IPPH instigated a strong scientific presence at Canada's largest annual public health conference through a landmark partnership with the Canadian Public Health Association, Public Health Agency of Canada (PHAC) and the Canadian Population Health Initiative signed in April 2005. This partnership has fostered a culture of evidence-informed action within the public health renewal agenda and increased responsiveness by the Institute to emerging PPH needs.
Initiative 2: Catalyzing the shift from describing determinants of health to an examination of pathways to health equity
Compelling data from many countries highlight persistent socio-economic gradients in health status, some of which reflect unfair yet avoidable inequities. Understanding the interplay among biological, social, cultural and environmental health determinants that produce these gradients is critical to improving our understanding of the pathways to health equity. This orientation towards health equity research builds on the solid foundation laid by the Institute in the early years to support research that describes, investigates and especially reduces disparities in health status as defined by socio-economic status, geography, race/ethnicity and/or gender.
IPPH has catalyzed research on health disparities within CIHR and with national partners and established the building blocks for health equity research through strategic investments in pilot projects, development grants for seed research and multi-year team grants. The Institute has created momentum for cross-institute collaborations through the Reducing Health Disparities Initiative. The Institute's efforts have resulted in a major increase in the production of knowledge on health disparities by Canadian researchers with noteworthy policy impacts and a vibrant research community that is well-positioned to respond to one of IPPH's current strategic foci: to understand pathways to health equity.
Initiative 3: Building the field of population health intervention research
As noted in the first international review and several recent reports and analyses of published literature, relatively little attention has been given to research on population health interventions.Footnote 7,Footnote 8 Operating within and beyond the health sector, these interventions include policy, program and resource distribution approaches that address the determinants of health and exert influence at organizational and system levels. Population health intervention research (PHIR) involves the production of knowledge about policy and program interventions that improve health at the population level and reduce inequities.Footnote 9
Our Institute has garnered international recognition for its approach to building the field. Through targeted investments, intellectual contributions at international symposia and strategic alliances focused on increasing the quality, quantity and use of PHIR, IPPH has stimulated novel theoretical and methodological advancements in this emerging field. The Institute co-leads the Population Health Intervention Research Initiative for Canada and is catalyzing the development of ethical principles and peer review guidelines for PHIR.
Outputs and Outcomes
IPPH used several data sources to identify outputs and outcomes for these three initiatives. All funding-related data and the bibliometric analysis were provided by CIHR Data and Analysis and Impact Assessment units, with additional data obtained through independent evaluations of major funding initiatives, surveys of trainees and reviews of mid-term, end-of-project and annual evaluation reports for specific funding competitions. All CIHR funding data are subject to limitations. Specifically, findings are based on a keyword search of the CIHR funding database. All theme 4-related data included herein have been validated by IPPH staff for relevance to the theme. This is because analyses conducted by IPPH demonstrated a 20–35% error rate when self-declared theme affiliation was used. This error rate includes both false-positive and false-negative affiliations. Multiple institute affiliations are possible for any project. As a result, the summary data for all institutes will add up to more than 100%.
Over the past 10 years, IPPH has led or co-led 60 strategic funding opportunities, including 21 priority announcements through CIHR's open competition. Through these funding opportunities, IPPH has invested more than $41 million and has partnered with all 12 of its fellow CIHR Institutes and three CIHR branches including the CIHR Ethics Office. By leveraging $27.7 million from other arms of CIHR and $13.1 million from external partners, the Institute has nearly doubled the funding for these competitions. IPPH's success in leveraging resources and partnerships demonstrates the relevance of our funding opportunities to partners within and beyond CIHR. The remaining $22 million in IPPH's strategic budget has been spent to support cross-pillar research and the priorities of other CIHR Institutes and branches and external partners. IPPH receives the same annual strategic granting budget as all CIHR Institutes, an amount that has grown to ~$8.5 million.
Figure 1: Percentage of total CIHR expenditures related to theme 4 research since 2000
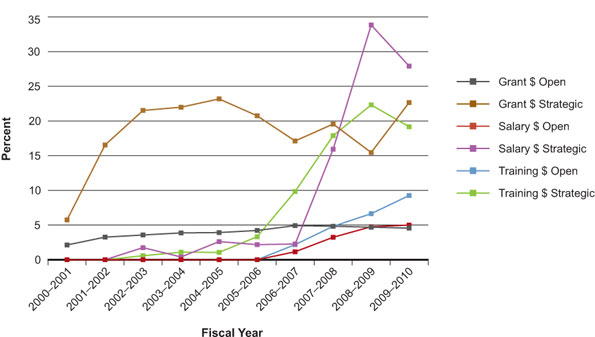
The consistently strong application pressure to IPPH's large strategic initiatives highlights the relevance of Institute-led funding mechanisms. Across CIHR, strategic grants in theme 4 research have grown notably from $11.2 million in 2001–2002 to $36.3 million in 2005–2006 and in 2009–2010, totaled more than $54 million.
Although steady gains were made in the proportion of theme 4 open grants awarded between 2000–2001 and 2009–2010 (by which time the number had more than tripled from 59 to 191), the expenditures have not grown over the past three years. As Figure 1 shows, the proportion of CIHR open grants awarded to theme 4 researchers has consistently been less than 5%. One possible explanation for this was identified in two reports on CIHR's peer review process for open grants. One report noted that health services and population and public health (PPH) peer reviewers rated applications an average of 0.5 points lower (on a scale of 0 to 4.9) than their medical counterpartsFootnote 10 and in both reports, different patterns in the nature of reviewer comments in these research areas relative to medical panels were highlighted.Footnote 10,Footnote 11
Initiative 1: Demonstrating scientific leadership for public health revitalization in Canada
Advancing knowledge
Despite some of the aforementioned challenges, compelling theme 4 research has been funded through CIHR's open competitions. Notably, there have been a few large-scale research grants funded such as the International Tobacco Control Policy Evaluation Project, which received one of the largest CIHR open grants ever awarded ($3.88 million). This research is advancing knowledge about the population health impacts of the world's first public health treaty, the World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC). Dr. Geoff Fong, an IPPH-affiliated researcher and his team are conducting comparative policy research in 20 countries about the effectiveness of the FCTC policies on curbing the global burden of tobacco use. They have produced more than 60 peer-reviewed publications and hold funding from 27 different agencies worldwide.Footnote 12 The team was recognized in 2009 with the CIHR-Canadian Medical Association Journal Top Canadian Achievements in Health Research Award.
In response to identified PPH research capacity gaps, IPPH made the first-ever CIHR investment in PPH research infrastructure when it funded mission-driven Centres for Research Development (CRD) across Canada in 2004 with a total investment of $16.8 million. The CRD program asserted the importance to health of research into the impacts of social and physical environments and created multi-year platforms for interdisciplinary programs of research. Several key informants in the program's mid-term evaluation applauded IPPH for their investment, describing it as "courageous", "strategic" and "audacious".Footnote 13
The seven CRD continue to yield significant research output. From 2003–2010, CRD-affiliated researchers produced more than 820 peer-reviewed journal publications with an average of 117 publications per centre (range=29 to 182 publications/centre).Footnote 14 The centre's leadership was a key criterion in peer review. It is clear from the publication patterns that centre directors are at the pinnacle of their respective fields and publishing in high-impact journals. For example, a recent Scopus database search found that Dr. Penny Hawe has published more than 30 papers since 2004, which have been cited an average of 13.6 times (444 total). Similarly, Dr. Louise Potvin has published more than 40 papers over the same time period, which have been cited an average of seven times (286 total). These publications are in addition to numerous policy briefs, book chapters and special reports.
Beyond the impacts of our funded researchers, the Institute has made a concerted effort to advance knowledge in this field by actively publishing on the conceptual foundations for PPH research and approaches to public health renewal in high-impact journals such as Epidemiology,Footnote 15 Canadian Medical Association Journal,Footnote 16 and Annual Reviews of Public Health.Footnote 17 The Institute also sponsored four peer-reviewed journal supplements in the Canadian Journal of Public Health (two in 2005, and one in each of 2006 and 2009) to lend coherence to the publication of findings from research funded under several IPPH strategic investments.
Other Institute initiatives to advance and exchange PPH knowledge have included the co-sponsorship of Café Scientifiques with the Public Health Agency of Canada (PHAC) on topics such as food security, global health and mental health and employment conditions. Cafés have been well attended (average 75 attendees) and achieve community outreach and citizen engagement. Further, since January 2003, IPPH has published 22 issues of POP News, a bilingual newsletter, which is distributed to the broader IPPH community (>1,200 people). The content is substantive and includes invited feature articles, profiles of funded researchers, book reviews and a newly developed student section.
Capacity building
Salary and training awards
In 2002 and 2003 IPPH made a multi-year investment in a separate pool of trainees funded by or affiliated with theme 4-related CIHR Strategic Training Initiative in Health Research (STIHR) programs. In total, 581 trainees (including 124 master's; 266 doctoral; 138 postdoctoral) involved in 16 STIHRs received support for training and career development, gaining valuable exposure to PPH research methods and theories. One such STIHR, led by Dr. Gilles Paradis, Director of the Quebec Population Health Research Network, is embedding training opportunities into 10 public health organizations in Quebec and engaging more than 50 mentors from six universities. The STIHRs, coupled with more accessible graduate programs in public health, have attracted students from a wide range of disciplines who may not otherwise have entered the field. Early strategic investments in training have yielded a substantial increase in open training awards, with steady increases seen over the past four years. The proportion of CIHR dollars awarded to theme 4 trainees has nearly doubled since 2007–2008 (Figure 1). A similar pattern can be seen for salary awards, demonstrating improvements in the capacity of theme 4 researchers to obtain these highly competitive awards. In 2009–2010, CIHR funded 18 open salary awards in theme 4 research ($920,000), compared to no awards in this field in its first five years.
Another pivotal achievement was a partnership between IPPH, PHAC and other partners to co-fund 15 Applied Public Health Chairs (APHC) in 2007–2008 thereby responding directly to recommendations from the first international review to address the gap in mid-career support. The Chairs program is remarkable in a number of ways. Its relevance to the public health renewal agenda resulted in a three-fold increase in IPPH investments by PHAC and other partners. This program has attracted researchers from disciplines as diverse as veterinary science, economics and geography and has coaxed some of Canada's best scientists to the field of applied public health research. This partnership also provided funding for some 112 graduate students in public health research. Between 2005–2006 and 2007–2008, IPPH contributed $3.2 million to training awards and $4.8 million to the APHC program, leveraging an additional $2.9 million and $10.5 million respectively.
Creating supportive PPH research environments
In addition to building individual researcher capacity, IPPH has funded research infrastructure such as the CRD, which have lured talented researchers and trainees to PPH research. Since 2004, the number of researchers affiliated with CRDs has grown four-fold to well over 200. While continuing to engage core public health disciplines such as epidemiology, the centres have also made major gains in interdisciplinarity by attracting social scientists and expanding the involvement of researchers from biology, physical and environmental sciences and the humanities. This has increased research and leadership capacity in PPH, particularly in underdeveloped regions of Canada.Footnote 14
The centres have funded 175 seed research projects, nearly half of which have resulted in applications for peer-reviewed funds (an underestimation, as recently funded seed projects have not had time to produce the results necessary to support a proposal). A total of 183 research grant proposals submitted to federal or provincial granting agencies by CRD researchers have been funded, the overall success rate for centre-affiliated research proposals averaging some 60% – higher than is typical for peer-reviewed funds.Footnote 14
The CRD have contributed significantly to critical changes in the PPH research landscape, including the establishment of several Schools of Public Health and Master's of Public Health (MPH) programs.Footnote 14 Four centres have collaborated on the delivery of annual Summer Institutes (led by IPPH and the Institute of Health Services and Policy Research). These capacity-building events have involved more than 280 trainees from across Canada since 2002. A survey of recent attendees found that more than two-thirds (n=42/62 respondents) are currently working in the field of PPH research or health services and policy research.
Summative evaluation data show that the CRD will leave a considerable legacy in sustainable research activities and infrastructure, the former through relatively autonomous groups that have acquired major research funding. Centres have leveraged more than $135 million in additional peer-reviewed research funds – more than eight times their original investment. Two CRD have obtained Canada Foundation for Innovation funding to sustain their research platforms, while several others have secured infrastructure support from their host institutions and existing funding partners by acquiring CRD status.Footnote 14
Informing decision making
The Institute has informed decision making by bridging PPH research with current policy and practice initiatives. It has deliberately embedded knowledge translation (KT) requirements in the majority of its strategic funding programs as an upstream approach to integrated KT.
Research and related activities led by IPPH-funded CRD are directly informing policies or policy changes. Key informants in the CRD evaluationFootnote 14 noted that the required co-governance model implemented by the centres and their decision-making partners supported KT by forging strong and sustained linkages between researchers and knowledge users. These structures formalized a vital link for all centres to provide scientific input on program and policy decisions. Centres have informed decision making across all levels of government in health and other sectors. For instance, the Centre Léa Roback in Montréal has informed local zoning changes through its research on fast-food accessibility, while the Canadian Centre for Health and Safety in Agriculture has influenced Manitoba's new traffic regulations to improve human safety when heavy farm machinery is moved.
IPPH has joined forces with other institutes to advance knowledge, inform decisions and provide practical evidence on emerging public health threats. One such partnership was the rapid-response research funding mechanism for public health services research on severe acute respiratory syndrome (SARS). Dr. Ross Upshur was funded through this mechanism and developed an ethical framework for pandemic influenza. The framework, which addresses the issues of health worker obligations, priority-setting, public health measures and global governance, has been adapted by the WHO in its guidance to member states and incorporated into pandemic plans in Canada, the United States, New Zealand and Europe. In direct response to an evidentiary need expressed by PHAC, IPPH recently led a rapid response call to support the study of public health and health care system interventions for H1N1 and their effects on vulnerable populations.
Initiative 2: Catalyzing the shift from describing determinants of health to an examination of pathways to health equity
The Reducing Health Disparities Initiative
IPPH and the Institute of Gender and Health co-led the Reducing Health Disparities Initiative, a cross-institute effort designed to generate research and build capacity to document, analyze and reduce health disparities. Early funding for developmental and pilot research was followed by larger, multi-year team grants. The Initiative has since been featured in a special issue of the Canadian Journal of Public Health.Footnote 18 Its flagship funding competition, Reducing Health Disparities and Promoting Equity for Vulnerable Populations Interdisciplinary Capacity Enhancement (ICE) grants, funded 20 teams for a total CIHR investment of $14.4 million. IPPH contributed nearly $3 million.
Advancing knowledge
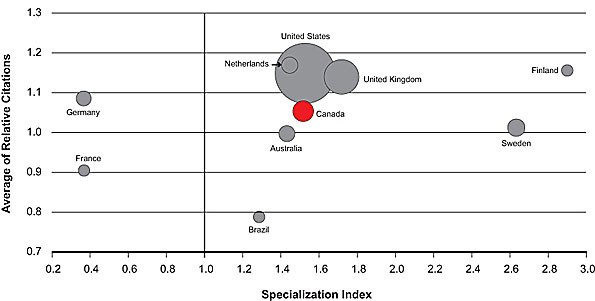
Bibliometric data provide a useful measure of advancing knowledge. In Figure 2, the circle size relates to the number of publications produced in the research area between 2000 and 2008. There has been a steady increase in the number of Canadian publications in health status disparities research over time, from 70 in 1997 to 261 10 years later in 2007. Canada now ranks third with 1,462 publications from 2000–2008. Final reports from 17 of the 20 funded ICE teams indicate that more than 430 journal publications have resulted from their research, suggesting that the teams have contributed substantially to these positive trends. Figure 2 shows the average of relative citations (ARC) and specialization index (SI) for publications in this field among the top 10 countries from 2000 to 2008. Canada scores above the world average of 1.0 on both indices (1.05 and 1.52, respectively) and ranks sixth among the top 10 countries for ARC and fifth for SI. An ICE team leader (Dr. Clyde Hertzman) was identified in the bibliometrics as being highly cited and the most published Canadian researcher in this field.
The literature in the area was identified through a set of U.S. National Library of Medicine Medical Subject Heading searches. The search may not be 100% specific or sensitive. The databases searched do not necessarily provide comprehensive coverage of all journals publishing in the area. The top 10 countries were ranked based on numbers of publications for the entire time period. ARC data were incomplete for 2008 and may underestimate the actual value.
Figure 2: ARC and SI for top 10 Countries publishing in health status disparities, 2000–2008
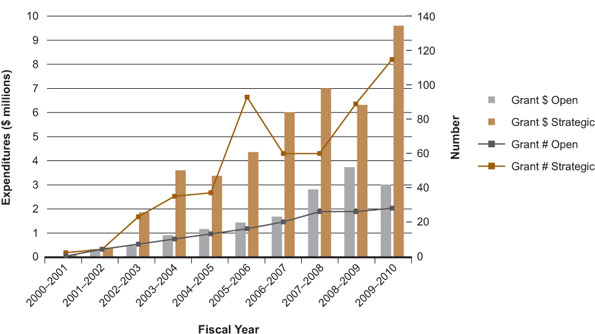
Another indicator of advances in knowledge is the ability of researchers to successfully compete for CIHR funds. An analysis of theme 4-funded projects suggests a steady increase in the number and amounts of funded health disparities/equity/inequalities research (Figure 3). Early investments of strategic funds seem to have increased successes in the open grants competition in this area with a doubling of open grant expenditures between 2004–2005 and 2009–2010. The implementation of funding mechanisms to address our current strategic plan led to an increase in strategic grants in 2009–2010; this may have temporarily drawn theme 4 researchers away from the open competition.
Figure 3: Health disparities/equity/inequalities-related theme 4 expenditures and number
of grants by fiscal year
Capacity building
An analysis of ICE teams found that, over the course of their grants, they had leveraged more than $40 million in additional funding from CIHR and other sources. This represents a significant return on investment in terms of building interdisciplinary research capacity, with every CIHR dollar invested resulting in nearly three dollars in additional funding.
The ICE teams developed a range of capacity building mechanisms, engaging more than 450 students, fellows and new investigators and creating innovative training platforms for research on vulnerable populations. Some teams built research capacity with community-based organizations while others offered seed grants to affiliated investigators to support data collection for subsequent research proposals. Some also integrated social science researchers by mentoring and providing co-investigator support for CIHR applications.
Informing decision making
IPPH-funded researchers in Canada made substantial intellectual contributions to the WHO Commission on Social Determinants of Health.Footnote 19 Two of the Commission's knowledge networks have strong Canadian leadership and involve researchers who were funded by the Reducing Health Disparities Initiative (Drs. Clyde Hertzman and Ronald Labonte). IPPH is a member of the Canadian Reference Group, which supported Canada's participation on the WHO Commission and is implementing national actions to reduce health inequalities.
ICE teams are working at the interface of research and practice. Dr. Cordell Neudorf, Chief Medical Health Officer for the Saskatoon Health Region, produced the highly acclaimed report Reducing Health Disparity in Saskatoon: From Analysis to Intervention,Footnote 20 touted by Canada's Commissioner, Monique Bégin, as a template for intersectoral and interdisciplinary collaboration. Its findings were presented to two senate subcommittees and the Parliamentary Subcommittee on Health and directly informed the Saskatoon Action Plan to Reduce Poverty. Dr. Theresa Gyorkos and her team conducted research in an impoverished area of Peru, where they worked with the national ministry of health and others to implement a delayed cord-clamping intervention. The initiative has significantly reduced infant anemia and supported hospital policy changes to reduce infant morbidity.
Some ICE teams have advanced knowledge on the ethics of working with vulnerable populations and linked intervention planning across health, legal and social service sectors. Dr. Stephen Hwang and a team of university- and community-based researchers described health status disparities of homeless adults; their work, including the 2007 Street Health Report,Footnote 21 has become a call to action to develop a comprehensive approach to homelessness in Canada. Dr. Elizabeth Saewyc and her team tackled sexual exploitation and marginalized youth. Their research has achieved international impact, as their Street Youth Survey analyses informed the National Youth Policy Institute of South Korea and their Runaway Intervention Project was singled out by the U.S. Agency for Healthcare Quality and Research as a promising intervention and was identified as an effective prevention and intervention strategy by the U.S. Office of Juvenile Justice and Delinquency Prevention.
Initiative 3: Building the field of population health intervention research
Advancing knowledge
There are increasing calls for PPH research that interrogates complex interventions within complex adaptive systems. Canadian scientists are making important contributions in this growing field of research redefining the fields of knowledge utilization and systems science, as recently featured in New Directions in Evaluation.Footnote 22 This CIHR-funded work on complexity science, research designs and theories for population health intervention research (PHIR) has attracted international attention.
Specifically, the team at the Population Health Intervention Research Centre, funded under the CRD program, pioneered an alternative way of standardizing an intervention in a cluster-randomized trial that allows interventions to adapt to context. The process potentially makes interventions more effective, while retaining the integrity of the randomized controlled trial (RCT) design.Footnote 23 This advance in theory and methods is being applied to design RCTs of neighbourhood renewal interventions in the UK and physical activity interventions in Germany. It is also being put forward as a best practice in obesity intervention design and evaluation.Footnote 24 The Centre's advances in complex PHIRFootnote 25,Footnote 26 led to an invitation to take part in WHO's Global Alliance for Health Policy System Research.
Such foundational theories and methods are essential for building the field of PHIR. Canadian scientists and IPPH are leading other important advances in this area. In 2006, 50 scientists and decision makers participated in a ground-breaking workshop that articulated the parameters of PHIR in Canada. An important outcome of the workshop was a supplement in the Canadian Journal of Public Health,Footnote 27 in which 19 leading Canadian researchers and stakeholders (including Chief Public Health Officer, Dr. David Butler-Jones) authored a suite of peer-reviewed papers that defined PHIR and identified gaps and opportunities for promoting excellence in this field.
Another workshop outcome was the launch of the Population Health Intervention Research Initiative for Canada (PHIRIC), a pan-Canadian initiative aimed at advancing the science of PHIR and strengthening Canada's capacity to fund, conduct and use this research. IPPH is the secretariat for PHIRIC, which serves as an ongoing platform for discussions among scientists and funding organizations on how to advance knowledge on population health interventions and its use. While PHIRIC represents a substantial investment of time, effort and money by all concerned, it has succeeded in creating a constituency of support for PHIR and has successfully mobilized considerable resources for PHIR as evidenced by the strategic funds allocated by several PHIRIC partner organizations, including the Canadian Population Health Initiative, PHAC and the Heart and Stroke Foundation of Canada (HSFC).Footnote 28 Efforts to sustain multi-year and dedicated investments in PHIR are needed to further build this field.
Opportunities to advance and exchange knowledge in this area were also fostered through an IPPH-led Funders Forum in 2009 and an international symposium on PHIR in 2010. IPPH-funded scientists are regarded as thought leaders for their catalytic field-building efforts in PHIR and have been invited to share the PHIRIC model with partners in the U.S., the UK, France and Australia. PHIRIC and IPPH are engaged in international consultations to provide input on framing the burgeoning field of PHIR through a Medical Research Council UK-led initiative.
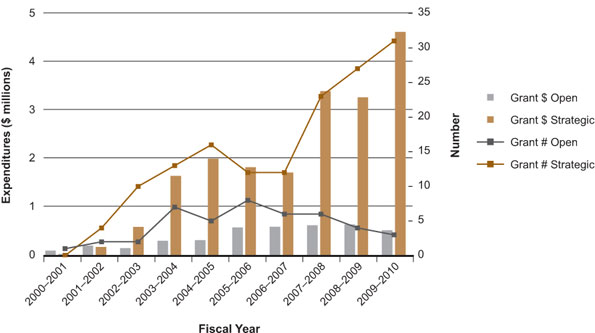
CIHR strategic investments in PHIR have increased two and a half times since 2006–2007. However, there has been extremely limited funding for theme 4-related PHIR received through open grants, with only three funded in 2009–2010 (Figure 4). A possible explanation could include a lack of appropriate funding mechanisms available to fund PHIR. IPPH is working with the CIHR research portfolio to develop urgently needed open-competition funding mechanisms and peer-review processes to support research in this field.
The increase in strategic funds is attributable in part to a novel Operating Grant for Intervention Research. This funding mechanism, co-led by IPPH and the Institute of Nutrition, Metabolism and Diabetes, directly responds to government priorities in chronic disease prevention, is structured to enable the study of rapidly unfolding interventions and includes peer review criteria appropriate for PHIR. A recent evaluation of funded projects found that more than 70% of recipients would not have been able to conduct their research on time-sensitive "natural experiments" without this grant funding. This suggests that, in the absence of this funding mechanism, many opportunities to capture timely policy- and program-relevant intervention data might have been missed entirely.Footnote 29
Figure 4: Population health intervention research-related theme 4 expenditures and number of grants by fiscal year
Capacity building
Closely linked to advancing knowledge is the capacity to fund, conduct and use PHIR. IPPH partners with organizations and scientists to facilitate capacity building efforts in this emerging field at multiple levels. To that end, capacity building strategies have been directed toward trainees through a targeted call for PHIR-related applications to the 2009 CIHR STIHR program. Three PHIR-related applications were renewed and three new ones granted. While it is too early for outcome data, these efforts show significant promise. Drs. Louise Potvin and Penny Hawe are creating robust research, ethics and KT training opportunities by building on their IPPH-funded CRD in partnership with the National Collaborating Centres (NCC) for Public Health. Dr. Roy Cameron's pan-Canadian approach to training links 66 mentors across nine provinces and three Schools of Public Health. The extensive training networks exemplified by these STIHRs are yielding new intensive and traditional courses on PHIR, stimulating innovation and the cross-fertilization of ideas and ensuring that trainees are exposed to leading mentors and training in this field of research.
Informing decision making
Many IPPH investments are enabling researchers to conduct highly relevant PHIR and inform decision making. Several teams funded through the Operating Grant in Intervention Research have directly influenced policy. Dr. Yves Couturier has worked with Quebec's provincial public health institute to study L'Approche École en Santé, a comprehensive health-promotion policy developed by the provincial ministries of Education, Recreation and Sports and Health and Social Services. His findings validated the policy as an evidence-based approach and informed support and training to implement the policy. Shirley Thompson and Jeff Gordon evaluated the Northern Healthy Food Initiative, a series of projects to improve food security in Northern Manitoba. Findings were presented to policy makers in seven provincial departments and have resulted in the implementation of local food charters.Footnote 29
Applied Public Health Chair-led research has directly informed policies and programs and set public health agendas in various provinces. Dr. James Dunn worked closely with municipal public health decision makers in Peel Region to develop and implement a tool for understanding the population health impacts of urban sprawl and the built environment. This tool is informing the region's urban planning processes. Dr. Jean Shoveller developed novel methods to document youth sexual health outcomes by geographies and provided unique insights into the influence of underlying population-level conditions on contraception choices. Her Youth Sexual Health Mapping Initiative informed plans for ongoing monitoring of indicators at the provincial level and within five health authorities in British Columbia (BC). Also in BC, Dr. Benedikt Fischer's research on the risk of hepatitis C virus transmission from the sharing of crack-use paraphernaliaFootnote 30 argued for safer crack-paraphernalia distribution programs. Despite controversy, a program has been implemented by the BC Centre for Disease Control, reframing the nexus between public health and harm-reduction agendas in the province.
Many APHC are developing and applying novel methods to support population health intervention planning. Dr. Alan Shiell is working with the Calgary Health Region to apply economic methods to a cost-effectiveness evaluation of a walkability intervention for Calgary neighbourhoods and with PHAC to advance economic analyses of upstream health interventions. Dr. Doug Manuel developed simulation models for estimating new cases of diabetes and the expected impact of population-based interventions for the disease. The resulting 2010 report,Footnote 31 co-published by the Institute of Clinical Evaluative Sciences and the Ontario Agency for Health Protection and Promotion, is informing provincial decision making for diabetes prevention and management.
IPPH is directly informing decision making related to PHIR through engagement with policy makers. John Frank, the former IPPH Scientific Director, was one of only two CIHR scientific directors to serve as a witness at the 2006–2008 hearings for the Senate Sub-committee on Population Health. The report, tabled in the Senate of Canada, recommends that CIHR and other relevant partners work to assess current investment in PHIR, determine an appropriate level of funding in this field and build on current capacity to develop innovative funding mechanisms.
Cross-initiative public health system impact and transformative effects
Since IPPH's strategic investments have been designed to work synergistically, this section describes the cumulative effects of the three initiatives in this report.
Public health system impact
Sounding the alarm and renewing Canada's public health system
Prior to any knowledge of SARS, IPPH led a study on the organization and funding of public health services in several countries that served as the basis for recommendations to strengthen Canada's public health system.Footnote 32,Footnote 33 Ratified at a national IPPH-led think tank in May 2003,Footnote 34 the recommendations have been integrated into national and provincial reports that are guiding public health system reforms. The same think tank resulted in the creation of the Canadian Public Health Association-led Canadian Coalition for Public Health in the 21st Century, whose membership includes 33 professional and non-governmental organizations that support a revitalized public health system.
The public health system impact of IPPH was recognized in the high-profile Naylor Report on SARS, which made reference to the Institute having "recently led a group of opinion leaders through a process to consider the future of public health and [for identifying] examples for [core public health] functions".Footnote 6 Mention in this important report to provide policy advice to the federal Minister of Health is a clear indication of the Institute's direct impact on urgent calls for public health system renewal. Further acknowledgement was made when the inaugural IPPH scientific director was invited to participate in the Special Public Health Task Force, which advised the Minister of Health on the establishment of PHAC (announced in the February 2004 federal Budget).
The Institute has also contributed to building broader public health workforce capacity in Canada. IPPH's Associate Director serves as co-chair of the Public Heath Human Resources Task Group, which advises the National Public Health Network Council on public health human resources development and ensures formal connections to front-line public health decision makers. Through the task group, IPPH has made notable contributions to developing guidelines to improve the quality and consistency of the MPH program, an analysis of options for the accreditation of MPH programs and Schools of Public Health and the establishment of Core Competencies for Public Health in Canada.Footnote 35
Creating national structures for knowledge translation and exchange
In early 2002, IPPH, in collaboration with Health Canada, conducted a comprehensive analysis of the issues and barriers related to PPH knowledge generation, dissemination, exchange and uptake.Footnote 36 This critical assessment informed the design of the NCC for Public Health program, a first-ever investment by PHAC in knowledge synthesis, transfer and exchange functions related to effective public health policies, programs and practices. The current and former IPPH scientific directors provide strategic guidance through the program's Scientific Advisory Council, bringing their expertise to bear on program development and evaluation and offering a means to further align KT and exchange structures for theme 4 research in Canada.
Transformative effects
Building a vibrant population and public health research community
Through strategic and collaborative investments, IPPH has raised the floor for PPH research and related KT in Canada. The Institute has transformed the PPH research community by nurturing a strong cadre of researchers who are highly productive, successful at leveraging peer-reviewed funds, committed to integrated KT, have better access to dynamic and interdisciplinary research environments and are engaged in training the next generation of researchers.
Synergies across the APHC, STIHR and CRD programs and the strategic linkages of researchers with the Schools of Public Health, are extending the impact of IPPH dollars and harnessing capacity to ensure that Canada's public health renewal is informed by the best available research. These synergies have catalyzed stronger and more diverse inter-university networks and suggest that capacity building for PPH research will be sustained at a higher level than ever before.
Beyond its financial investments, IPPH has shared its expertise across CIHR, providing leadership for a theme 4 research perspective. These intra-agency actions are complemented by IPPH's significant contributions to program and policy actions, which are revitalizing public health in Canada.
Innovation in funding and peer review for theme 4 research
Funding mechanisms and peer review criteria designed specifically for theme 4 are essential to help CIHR realize its cross-theme transformative mandate. IPPH has developed innovative funding mechanisms that have been adopted by other organizations and CIHR Institutes and initiatives, providing strong endorsement for its approach to building PPH research and KT capacity. The CRD program, for example, has been the model for at least two CIHR programs: the Centres for Population Health and Health Services Research Development in HIV/AIDS and the Centres for Research Development in Gender, Mental Health and Addiction. Key informants have noted that the Canadian Partnership Against Cancer's new Coalitions Linking Action and Science for Prevention Program implemented a similar model.Footnote 14
IPPH is also influencing other funders to use novel mechanisms for PHIR. Early successes include the integration of the Institute's intervention funding tools with other agencies such as the Robert Wood Johnson Foundation and PHAC in the design and peer review of its Innovation Strategy to support intervention studies on mental health and obesity. The Institute has partnered twice with the HSFC on research examining the relationship between built environment interventions and health and has supported the development of the HSFC's peer review criteria in PHIR.
Stalwart leadership in health equity and global health research
IPPH has been a stalwart leader in advancing health equity, PHIR and global health research – areas that, historically, have not been well-funded through CIHR's open competition. Without the strong foundation laid by IPPH's strategic funding and collaborations to foster research and build capacity in these areas, Canada's contributions to the science and impact of these fields would not be what they are today.
IPPH has directly contributed to CIHR's mandate to improve the health of Canadians and the global community. The Institute's involvement since 2001 as CIHR's representative on the Global Health Research Initiative (GHRI) Steering Committee has provided much-needed continuity in renewing global health research capacity in Canada. This unique initiative, which involves departments and agencies responsible for health, health research and development assistance, has enabled innovative global health research, capacity building and KT programs that have forged robust partnerships between researchers in Canada and low- and middle-income countries (LMICs). This Institute has advised on more than 10 global health research programs, including a portfolio of pilot, development, team and operational research grants.
A watershed event in the history of global health research funding in Canada was the creation of the GHRI-Global Health Teasdale-Corti Team grants in 2006. These teams aimed to build capacity for Canada and LMIC institutions to effectively undertake programs of research. The call led to an unprecedented 259 letters of intent and 14 teams funded, totaling $20.8 million (CIHR investment $12.9 million) – the single largest multi-year funding for global health research by CIHR through the GHRI. IPPH, through its involvement in GHRI, has helped develop principles that integrate research, capacity building, ethics and KT and encourage bi-directional learning and mutually respectful collaborations between Canadian and LMIC researchers. These principles are reflected in global health research funding programs such as the Teasdale-Corti Team grants.
One of the most transformative impacts of the Institute's leadership, however, has come from its direct role in institutionalizing global health research in Canada. IPPH helps CIHR fulfill its mandate by providing expert advice and creating sustainable partnerships that fund global health research and integrate capacity building, KT and ethics. The Institute has informed the design of novel CIHR global health funding programs and granting policies, including the development of an explicit organizational policy change in the CIHR Grants and Awards Guide whereby all CIHR funding competitions must include consideration of global health research.
The Institute has increased the visibility and legitimacy of global health within CIHR and universities as reflected in Roadmap's explicit recognition of global health research. In 2009, IPPH led development of the CIHR global health research strategy. The strategy is intended to bring further focus and coherence to CIHR's global health initiatives and optimize contributions for Canadian researchers who collaborate with LMICs on research into the health and health-system problems of these countries. These collective efforts have placed global health research squarely on the Canadian research landscape and are ensuring that it stays there. On behalf of CIHR, IPPH's Scientific Director, Dr. Nancy Edwards, has brought a population health lens to the working paper series of Grand Challenges Canada and guided the framing of strategic research investments for the Global Alliance on Chronic Disease.
Going Forward
In keeping with its mandate, IPPH is maintaining focus on the interplay of biological, social, cultural and environmental determinants while also examining changes in this interplay across the life course and through major societal transitions. Canada's scientists have contributed significantly to the field of determinants of health research across multiple health issues and populations.
Building on these foundations, IPPH is focusing more than ever on the emerging field of population health intervention research (PHIR) and the study of how micro- and macro-environments intersect to enhance equities or reduce inequities in the health of populations. This new focus is consistent with many national and international calls for action to improve health equity. Our scientific community is poised to significantly advance the field of PHIR over the next decade, working with decision makers who are shaping whole-of-government policies to improve population health and reduce inequities. IPPH is well-positioned to provide the leadership required to advance this science, including its methodological, theoretical and ethical foundations and its application in relevant sectors.
Over the past 10 years, IPPH has learned many important lessons within the transformative agenda that defines CIHR. These lessons, several of which are described below, require ongoing attention as the Institute implements its current strategic plan. IPPH has laid critical groundwork for research excellence in PPH in Canada; however, continued scientific advancements in pathways to health equity, population health interventions and implementation systems for these interventions, will require scientific progress and stalwart leadership on the following fronts.
Identify substantive priorities that align with IPPH's strategic plan and Roadmap
Unlike many other institutes, whose mandates cover specific health issues, diseases or populations, IPPH emphasizes a population health approach and focuses on health equity and population health interventions. As such, the Institute responds to emerging priorities and addresses substantive topics including obesity prevention, the built environment, H1N1 and mental health in the workplace. IPPH also allows a focus on future-oriented health concerns such as climate change and chronic diseases in LMICs, fulfilling a critical public health role.Footnote 4 This approach, however, has limitations. For example, the variability in substantive topics may make it more challenging to demonstrate a return on research investment on specific health issues. In consultation with its Institute Advisory Board (IAB), IPPH is developing a mixed approach to sustain investments in substantive priorities that align with Roadmap and partnership opportunities, alongside responsive investments that are consistent with the societal role of public health.
Infrastructure in the form of data platforms, scientific capacity and strategic partnerships within and outside of the health sector
The data infrastructure required for PHIR includes longitudinal cohort studies, multi-level population-based data systems, cross-sectoral record linkage and comparative policy data. Despite promising achievements, much more is needed to extend this infrastructure to facilitate large-scale PHIR. IPPH is engaged in cross-institute dialogue around solutions for data harmonization.
The Applied Public Health Chairs (APHC) and the Strategic Training Initiative in Health Research (STIHR) are an important extension of earlier collaborative capacity building investments in PPH research and reflect the Institute's emphasis on PHIR. Resulting increases in capacity have led to international recognition. IPPH and its scientists are participating in international scientific events designed to interrogate the foundations of PHIR and the implementation systems in which interventions are delivered.
To advance the PHIR strategic priority, IPPH continues to forge strategic partnerships with provincial ministries, public health agencies and other research funding organizations within and outside the health sector. IPPH's partnership with Public Health Agency of Canada (PHAC) remains critical in determining, for instance, how to optimally support PHIR and achieve the scale-up of promising interventions. The Institute will further build linkages with the National Collaborating Centres (NCC) with the goal of developing sustainable mechanisms for translating research into public health policy and practice.
A growth area for the Institute is to develop a greater understanding of the economic impacts of population health interventions. Institute involvement in an ongoing PHAC-led dialogue will guide methods and tools development to inform evidence on the costs and economic impacts of population health interventions in Canada – with a focus on social determinants and health inequities.
Expanding partnerships beyond the health sector will enable IPPH to deliver on two strategic priorities: population health interventions and implementation systems. IPPH has already garnered interest from the international research community through invited presentations at the Centers for Disease Control's Annual Conference for Centers for Prevention Research and the U.S. Agency for Healthcare Research and Quality-sponsored invitational conference on scaling-up. Building on these efforts, IPPH is exploring joint international funding collaborations that will provide a scientific platform for comparative PHIR.
Knowledge synthesis approaches that reflect the new science of population health interventions and a knowledge translation framework oriented towards systems change
An orientation towards research on health equity, population health interventions and implementation systems also signals the need for parallel advances in the science of knowledge translation (KT). The IPPH KT plan outlines the expansion and integration of knowledge synthesis approaches for PPH research and the creation of funding mechanisms to expedite research on ways to scale-up population health interventions across sectors. Together with CIHR's KT Branch, the Institute is developing a knowledge-to-systems change framework for population health improvements. With guidance from its IAB and other key decision-making partners, IPPH is reviewing other CIHR models for integrated KT, such as Partnerships for Health System Improvement and Best Brains exchanges, to determine their utility and fit with public health. One promising option is to build on existing links to the Pan-Canadian Public Health Network Council, which brings together chief medical officers and deputy ministers of health to collaborate on ways to improve public health in Canada.
A population health ethics framework that guides choices about population health interventions and their potential scale-up
To support theoretical and methodological innovation, the Institute is fostering the development and refinement of ethical frameworks for population health interventions in Canada and globally. IPPH is ideally positioned to support CIHR's ethics mandate by contributing to areas such as ethical reflection on the goals and social implications of PPH research. In 2009, the Institute implemented a highly successful virtual journal club and is now developing a series of case studies on ethical issues underlying population health interventions, with PHAC, the NCC on Healthy Public Policy and the CIHR Ethics Office. The Institute is also working with this Office to design funding mechanisms for research in this field.
Funding mechanisms that support exceptional science, coupled with peer-review mechanisms that enable its identification
CIHR has championed theme 4 research through its strategic priorities and made some important achievements in building supportive funding mechanisms. Several important challenges remain, as reflected in indicators such as overall funding allocations to this research at CIHR relative to other areas of investment, the mix and mandates of peer review committees for the open grants competition and the qualitative differences in reviewer feedback on theme 4 research.Footnote 6,Footnote 10 For CIHR to fully achieve its transformative agenda, IPPH must continue to influence peer review reform.
IPPH is experimenting with funding models for PHIR with internal and external partners. The Institute's new programmatic research funding opportunity, launched in early 2010, will be evaluated for its potential integration into CIHR's suite of open grant funding tools. The Population Health Intervention Research Initiative for Canada (PHIRIC) has developed peer review criteria for PHIR that are currently being pilot-tested. Developing fit-for-purpose peer review criteria is an important area for ongoing development and receives careful consideration in all IPPH strategic funding opportunities.
Scientific leadership for the health of Canadians
Current IPPH strategic priorities are well-aligned with Roadmap with a shared focus on improving health equity, chronic disease prevention and addressing global threats. The Institute will continue to exercise its leadership and catalytic roles by advancing knowledge of population health interventions and the biological, social, cultural and environmental determinants of health equity. However, as the 1999 National Health Forum report concluded, a shift in health research funding remains critical "to create an appropriate balance between research on non-medical determinants and basic and clinical research".Footnote 37 While research funding gains have been made, IPPH's integrative mandate will only be fully realized through its own ongoing efforts with CIHR and other institutes to identify optimal ways to foster leading-edge theme 4 research. This will be essential for CIHR to achieve its transformative agenda. IPPH's scientific leadership is pivotal to ensuring an evidence-informed public health system in Canada and ultimately the future health of Canadians.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
IPPH specific
| APHC | Applied Public Health Chairs |
| ARC | average of relative citations |
| BC | British Columbia |
| CRD | Centres for Research Development |
| FCTC | Framework Convention on Tobacco Control |
| GHRI | Global Health Research Initiative |
| HSFC | Heart and Stroke Foundation of Canada |
| IAB | Institute Advisory Board |
| ICE | interdisciplinary capacity enhancement |
| KT | knowledge translation |
| LMIC | low- and middle-income country |
| MPH | Master's of Public Health |
| NCC | National Collaborating Centres |
| PHAC | Public Health Agency of Canada |
| PHIR | population health intervention research |
| PHIRIC | Population Health Intervention Research Initiative for Canada |
| PPH | population and public health |
| RCT | randomized controlled trial |
| SARS | severe acute respiratory syndrome |
| SI | specialization index |
| STIHR | Strategic Training Initiative in Health Research |
| WHO | World Health Organization |
- Date modified: