Internal Assessment for 2011 International Review - CIHR Institute of Human Development, Child and Youth Health
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures
- Figure 1: Percentage of CIHR overall expenditures related to IHDCYH-relevant research, by fiscal year
- Figure 2: Specialization index and average of relative citations for top 10 countries publishing in reproduction, prenatal development and maternal health, 2000-2008
- Figure 3: Relative change in number of publications on child and youth health, Canada versus rest of the world, 1990-2008
- Figure 4: Trend in number of publications on child and youth health research in major medical journals, Canada versus rest of the world, 1990-2009
- Figure 5: Mean number of citations of publications in child and youth health, Canada versus rest of the world, 1990-2006
Mandate and Context
The Institute’s origins
Mothers and children are usually healthy and, other than neonatal intensive care, contribute little to the escalating costs of the health care system. With low and declining rates of fetal, infant and child morbidity and mortality, it seems difficult to argue that more strategic research is "needed" in reproductive and child health. But the preconceptional health of parents, the biological processes underlying normal and abnormal embryonic and fetal development, preterm birth, fetal growth, prenatal and postnatal cognitive and behavioural development, and the early origins of adult chronic diseases are important areas of health research that are unlikely to receive high priority for funding in an organ-based, disease-based or theme-based institute.
In other words, the process of development - i.e., the transition across successive stages of the life course - was likely to be ignored unless CIHR created an institute devoted to this area. To this end, the existence of the National Institute of Child Health and Human Development, within the U.S. National Institutes of Health structure, provided strong support for the relevance of such an institute within the newly developed CIHR.
Mandate and early history
The wording of IHDCYH’s official mandate, as proposed by the CIHR Interim Governing Council, was: "The Institute of Human Development, Child and Youth Health supports research to enhance maternal, child and youth health, and to address causes, prevention, screening, diagnosis, treatment, short- and long-term support needs, and palliation for a wide range of health concerns associated with reproduction, early development, childhood and adolescence." Although the official mandate was quite broad, the Institute leadership focused from the beginning on developmental processes and transitions in the life course rather than on specific organs or diseases.
Since its inception, IHDCYH has seen its strategic focus as the process of development (biological, behavioural and social), rather than as the myriad diseases that can afflict mothers, children and youth.
When IHDCYH was created, Canada had a vibrant, internationally recognized community of researchers in the areas of IHDCYH’s mandate, including:
- Reproductive and developmental biology
- Maternal-fetal endocrinology and physiology
- Perinatal epidemiology
- Perinatal and pediatric randomized controlled trials (RCTs)
- Developmental psychology, child psychiatry and neuroscience
IHDCYH’s early funding initiatives built on these existing strengths, rather than filling gaps. IHDCYH’s leadership recognized the need to use its strategic budget for more than merely extending the Open Operating Grant Program; the budget was used as well to break down barriers and encourage (or even require) collaboration among investigators across the four research themes: biomedical, clinical, health services and population health.
The Institute’s first Scientific Director was Dr. John Challis, a maternal-fetal endocrinologist and physiologist from the University of Toronto. Dr. Michael Kramer, a pediatrician and perinatal epidemiologist, was chair of the Institute Advisory Board. In May 2003, Dr. Challis left his position after two years. IHDCYH was the first CIHR Institute to change leadership when Dr. Kramer was named Scientific Director in May 2003 (interim until November 2003). In May and June 2004, assistant directors were hired at McGill University (Dr. Anne-Cécile Desfaits) and in Ottawa (Louise Poulin), and the Institute began to re-exert leadership in the reproductive and child health research community.
Institute Priorities
First strategic plan: 2001-2005
IHDCYH developed its original strategic plan with the help of Institute Advisory Board (IAB) members, five standing committees and a national planning retreat that included researchers, non-governmental organizations, federal and provincial governments and industry. The result was six strategic priorities:
- Pre- and postconceptional reproductive health
- Fetal growth and preterm birth
- Prevention of congenital anomalies
- Developmental trajectories of children and youth
- Causes, prevention and treatment of acute and chronic illness in children and youth
- Reproductive aging
The plan was to launch requests for applications (RFAs) to support team grants in all six priorities, with required participation from multiple research themes and substantial funding ($750,000 per grant per year for five years).
The philosophy underlining our strategic approach emanated from a need to develop a distinctive niche among the other institutes, as well as from a belief that strategic budgets would increase to $20-25 million a year. That amount would provide funding adequate not only to support several large team grants in each of the six strategic priorities, but also to allow other investments, including capacity building, knowledge translation (KT) and ethics. Thus, IHDCYH did not actively seek or expect co-funding partnerships with other CIHR Institutes.
After the first year or two, however, the Institute’s strategic budget began to plateau, and it became fiscally impossible to implement the strategic plan as envisioned. IHDCYH’s commitment of funds for five-year grants forced the leadership to decrease the size of team grants awarded in subsequent RFAs (from $750,000 per year to $500,000 per year maximum) and to search more actively for both internal and external funding partners. Thus, IHDCYH’s third multidisciplinary team RFA (Healthy Developmental Trajectories) included participation by four other institutes: the Institute of Gender and Health (IGH), the Institute of Neurosciences, Mental Health and Addiction (INMHA), the Institute of Nutrition, Metabolism and Diabetes (INMD) and the Institute of Population and Public Health. It also included an external partner, Autism Speaks. Conversely, IHDCYH began to partner on strategic initiatives led by other institutes: a large team grant in pediatric palliative care (RFA led by the Institute of Cancer Research, or ICR) and smaller grants in the areas of child obesity (with INMD), health inequalities (with IGH) and tobacco control (with ICR and INMHA).
Response to 2006 International Review
Another key aspect of IHDCYH’s first five years was the first International Review. Although a detailed evaluation of the individual institutes was not a central focus of the 2006 International Review Panel Report, the panel did make several recommendations concerning IHDCYH. These included greater investment in research on birth defects and mental health, more partnerships and improved incorporation of KT activities in our strategic initiatives.
Each of these recommendations has been acted upon. Birth defects are a central focus of a recent RFA on environmental contaminants and reproductive health. Mental health has become a major component of one of IHDCYH’s key initiatives (see Key Initiatives section). IHDCYH’s numerous partnerships are highlighted in a separate section, and KT accomplishments are summarized in the sections on informing decision making and on health system and economic impacts.
Second strategic plan: 2006-2010
IHDCYH’s second strategic plan was elaborated between April and November 2005. The process included interviews with the scientific directors of several other institutes, small focus groups of invited researchers and other stakeholders in Vancouver, Toronto, Montreal and Halifax, and regional forums for larger groups in Calgary and Ottawa. In addition, affiliated researchers from IHDCYH’s extensive electronic mailing list were encouraged to submit ideas for strategic priorities and other ways of supporting our research community.
A planning meeting was held in October 2005 with selected researchers, other stakeholders and the IAB. Several new areas were targeted for strategic investment that had not been included in IHDCYH’s first strategic plan: the physicochemical environment, child disability, intentional and unintentional injury and maternal health.
In addition, the importance of integrated (as opposed to end-of-grant) KT was reinforced as key for fulfilling IHDCYH’s mandate to improve the health and health care of mothers and children. This meant ensuring participation by non-researcher decision makers including clinicians; federal, provincial and territorial government policy makers; and nongovernmental organizations from the general community. We not only involved these decision makers in the planning of the research initiatives, but also, where possible, as members of the team that would carry out the research.
This increased emphasis on KT and external partnerships was a direct response to two key recommendations of the 2006 International Review.
By late 2006, IHDCYH had recognized the importance of building capacity in several key gap areas relevant to its mandate, particularly those involving ethics, KT, health and the environment, and health services and policy research (HSPR). Since then, IHDCYH has launched priority announcements for New Investigator Awards in these areas. We have succeeded in funding such awards in ethics, KT and environmental health, but not in HSPR. Moreover, despite the requirement for multidisciplinary collaborative research teams in IHDCYH’s RFAs from 2001-2005, it was quite clear that themes 1 (biomedical research), 2 (clinical research), and 4 (population health research) were well represented on the funded teams, whereas theme 3 (HSPR) was virtually absent from them. Canada’s weakness in reproductive and child HSPR is a key target of IHDCYH’s current and future strategic investments (see Going Forward section).
Alignment with Roadmap: fall 2009
In fall 2009, IHDCYH’s leadership aligned the Institute’s strategic priorities as closely as possible with those of Roadmap, CIHR’s overarching strategic plan for 2009-2014. This alignment did not require any fundamental modifications to our strategic priorities, but rather was achieved by bundling closely related priority research topic areas and cross-cutting themes. The result was four priority areas:
- Reproductive, prenatal and maternal health
- Neurocognitive and behavioural development and mental health of children and youth
- Chronic disease (focused on obesity, asthma, childhood disability and the developmental origins of adult chronic disease)
- Intentional and unintentional injury
The alignments also resulted in four cross-cutting priority themes:
- The social environment
- The physical environment
- Health services
- Aboriginal and other vulnerable populations
Chronic disease, mental health, health services and Aboriginal/vulnerable populations line up directly with three of Roadmap’s five strategic priorities. In addition, intentional injury (domestic violence, child abuse and suicide) and unintentional injury (especially motor vehicle accidents linked to alcohol or drug use) are closely linked to mental illness. Finally, exposure to environmental contaminants is explicitly mentioned in Roadmap among threats to health.
IHDCYH’s strategic priorities align well with those of CIHR’s Roadmap.
Key Initiatives
Process
When IHDCYH plans new strategic initiatives, Institute Advisory Board (IAB) members and other researchers with relevant expertise are invited, along with potential funding and decisionmaking partners and other stakeholders, to a consensus workshop with three major goals:
- Identify knowledge gaps and priorities within the given research area
- Propose broad research questions that should be addressed by a request for applications (RFA) in that area
- Choose the funding tools and develop a blueprint for the RFA
Following the consensus workshop, the IHDCYH leadership (Montreal and Ottawa staff and selected members of the IAB) and internal and external funding partners put together a writing team that helps develop the text of the RFA, which is then launched according to standard procedures within CIHR’s Research Portfolio and Finance Branch.
Rather than describe individual RFAs, the remainder of this section of the report will focus on two key initiatives that we believe have had a major impact on the Canadian research landscape in reproductive and child health. These initiatives have led to RFAs to fund multidisciplinary, multi-theme collaborative research in areas where such research did not previously exist, resulting in landmark research publications, increased research capacity and an enhanced profile of Canadian health research and researchers on the international stage.
Initiative 1: Reproductive health
IHDCYH began its program of multi-theme collaborative team grants with its first RFA, Healthy Gametes. We encouraged researchers from all four research themes to work together, usually for the first time, in an integrated program of research involving multiple academic institutions and multiple disciplines. After the funding expired for these teams, IHDCYH organized an end-of-grant workshop to present and discuss the research results. Evident at the workshop was not only the quality and quantity of the research accomplished by the teams, but also the extent to which investigators from diverse themes and disciplines influenced the directions and breadth of the research.
The success of this endeavour went well beyond conference presentations and high-quality publications. It also united the research community. This cohesion resulted in the funding of three new training programs in reproductive health research: two IHDCYH-funded Strategic Training Initiative in Health Research (STIHR) grants in reproductive health in the STIHR renewal round of 2008 and a reproductive biology training program in five academic institutions in the province of Quebec: the Réseau québécois en reproduction, co-funded by the Natural Sciences and Engineering Research Council (federal) and the Fonds québécois de recherche sur la nature et les technologies (provincial).
The now-unified reproductive health research community in Canada was instrumental in helping IHDCYH develop its recently funded RFA on environmental contaminants and reproductive health in collaboration with Health Canada. Under this RFA, two large multidisciplinary teams are investigating the adverse reproductive health effects of two endocrine-disrupting chemical contaminants that are highly prevalent in the environment: phthalates and brominated flame retardants. The outcomes studied include infertility, sexual dysmorphisms, other congenital anomalies and fetal growth and development.
This initiative clearly responds to the 2006 International Review recommendation to increase our funding in the area of congenital anomalies.
The partnered collaboration is a good example of IHDCYH’s emphasis on integrated knowledge translation (KT). Some of the basic biomedical research in this RFA will be carried out in Health Canada laboratories in Ottawa, thus ensuring that the results of the research inform Health Canada’s regulatory decision making in the area of chemical contaminants.
IHDCYH funding has helped unify Canada’s reproductive health research community through multidisciplinary teams and training programs.
Initiative 2: Behavioural development, mental health and addiction
IHDCYH’s initial RFA in this strategic area funded three large, multidisciplinary team grants in the area of healthy developmental trajectories. The teams cover a wide range of priorities for IHDCYH, one each on the effect of community and family influences on child development, the development of aggressive and antisocial behaviour and developmental trajectories in autistic children. In addition, three of the STIHRs funded by IHDCYH, one in the initial round (Pain in Children) and two in the renewal round (Autism, Reproduction and Early Development) have been related to this strategic domain.
The Academy of Finland has been a dynamic partner with IHDCYH in our recent strategic initiatives in child and youth mental health and addiction. In 2008, the Academy launched a major new initiative in child and youth health, with an emphasis on mental health. IHDCYH helped the Academy define the initiative and recruited other Canadian partners (the Alberta Centre for Child and Family Health Research, Alberta Innovates - Health Solutions, then called the Alberta Heritage Foundation for Medical Research, and the Norlien Foundation) to launch RFAs in the areas of early origins of mental illness and early origins of addiction. Two Canada-Finland teams were funded under the first of these RFAs. The second RFA (addiction) is currently awaiting peer review of the final applications.
In May 2010, in collaboration with the Institute of Gender and Health and the Institute of Aboriginal Peoples’ Health (IAPH), IHDCYH launched an RFA on maternal health entitled Maternal Health: From Preconception to the Empty Nest. As its title implies, this RFA focuses on the health of the mother herself, including maternal psychological and mental health. Unusual for CIHR, the RFA combines three funding tools: catalyst grants, knowledgeto-action grants and emerging team grants.
IHDCYH is currently working with the Mental Health Commission of Canada, the Institute of Health Services and Policy Research, the Institute of Neurosciences, Mental Health and Addiction and IAPH, as well as representatives from provincial governments and non-governmental organizations, to develop an RFA that centres on the development and testing of new models for improving access to services for children and youth with behavioural and mental health problems. This is an unusual initiative for IHDCYH and CIHR, because it involves sectors outside health, including social services, education and justice. This is one of IHDCYH’s first forays into multi-sectoral research but, given the grossly inadequate access to services for children and youth with behavioural and mental health problems and the resulting long waiting lists, involvement of multiple sectors is essential for developing and testing new service models. The RFA will be launched in the 2011-2012 fiscal year.
As recommended by the 2006 International Review, IHDCYH has made major investments in research on child development, mental health and addiction.
Outputs and Outcomes
Advancing knowledge
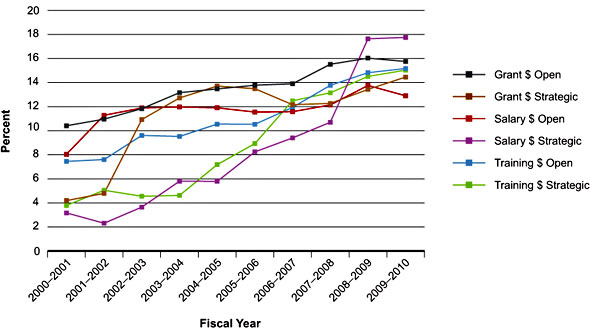
As shown in Figure 1, grants and awards funding in reproductive and child health has increased substantially since the creation of CIHR in 2000-2001. The data are expressed as percentages of overall CIHR expenditure in each category and thus demonstrate the relative growth of reproductive and child health research. These data show continued growth in open and strategic funding of grants, salary awards and training awards. In dollars, funding from 2000-2001 to 2009-2010 increased from $25.7 million to $73.8 million for open grants, from $1.3 million to $34.6 million for strategic grants, from $2.0 million to $2.3 million for open salary awards, from $0.1 million to $2.0 million for strategic salary awards, from $2.2 million to $8.1 million for open training awards and from $0.1 to $2.7 million for strategic training awards.
Figure 1: Percentage of CIHR overall expenditures related to IHDCYH-relevant research, by fiscal year
Given the increase in funding, it is not surprising that the number of Canadian publications related to IHDCYH’s mandate has also increased. Much research published by Canadian investigators in reproductive and child health is funded by sources other than CIHR and some is likely to be unfunded. Thus, caution is advised in inferring a direct causal relationship between CIHR (or IHDCYH) funding and Canadian publications.
Separate bibliometric analyses were conducted for reproductive health and for child and youth health. The former was carried out in a standard way across all institutes. To assess Canadian publications in child and youth health, we engaged a consultant. These two analyses were carried out simultaneously but used different methodologies.
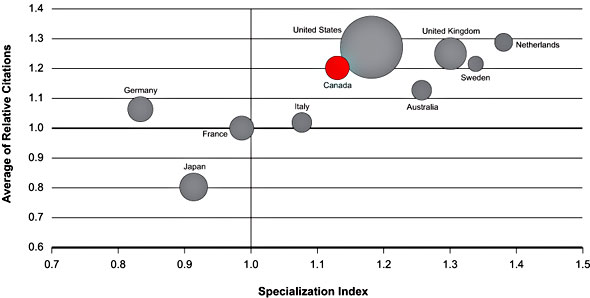
The bubble graph in Figure 2 shows three features of Canadian publications in reproductive health from 2000-2008, compared with the nine other leading countries: the average of relative citations (ARC), the specialization index (SI) and number of publications (size of the bubble).
ARC denotes the average number of citations in the two years following publication relative to the world average (=1.0). SI is a measure of the proportion of a country’s publications in the chosen area (here, reproductive health) relative to the world average (=1.0). Thus, Canada falls about 20% above the world average for ARC and about 14% above average for SI. The graph clearly demonstrates Canada to be one of the world’s six leading countries (along with the U.S., the UK, Australia, Sweden and the Netherlands) for SI and ARC in reproductive health research. For total number of publications from 2000 to 2008, the figures were 15,832 for Canada versus 116,662 for the U.S.
Figure 2: Specialization index and average of relative citations for top 10 countries publishing in reproduction, prenatal development and maternal health, 2000-2008
Canada’s publication record in child and youth health has been even more impressive. Figure 3 shows the relative change in number of publications (with 1990 as baseline) in this area between 1990 and 2008 from Canada versus the rest of the world. The figure shows an increase across the globe, but the rise in Canada is clearly higher than in the rest of the world. The total world absolute number of publications in child and youth health in 2008 was 87,062, of which 3,001 (3.4%) included one or more Canadian authors.
Figure 3: Relative change in number of publications on child and youth health, Canada versus rest of the world, 1990-2008
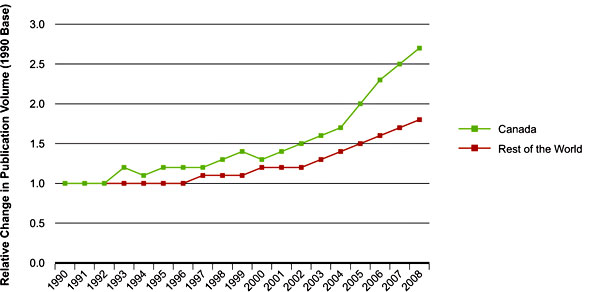
Figure 4 shows the relative trend (versus 1990) in number of publications on children’s health published in the following four major medical journals: New England Journal of Medicine, Lancet, Journal of the American Medical Association, and British Medical Journal. Canada has increased its number of publications since 1990, despite a steady and substantial decline in the rest of the world. As a consequence, Canada’s percentage of world publications on child and youth health in these journals rose from 2.6% in 1990 to 4.8% in 2009.
Figure 4: Trend in number of publications on child and youth health research in major medical journals, Canada versus rest of the world, 1990-2009
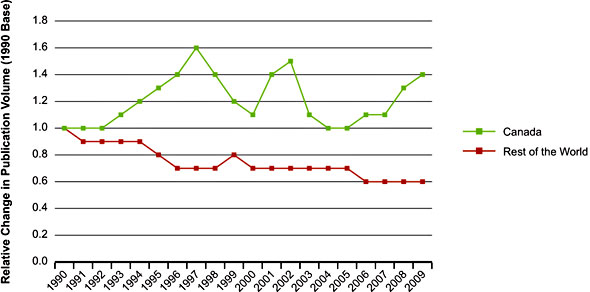
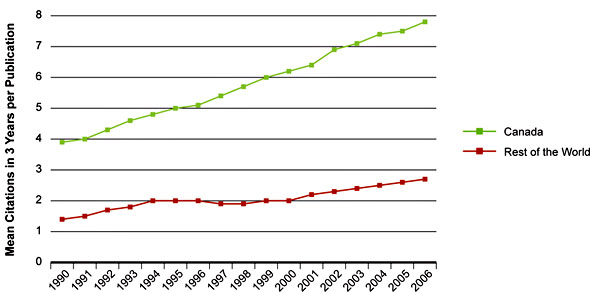
Figure 5 shows the trend in mean citations, within three years of publication, per article related to child and youth health published by authors from Canada versus the rest of the world from 1990 to 2006 (instead of 2008, to allow three full years for citations through the end of 2009). Although the number of citations has increased slightly in the rest of the world, the rate of increase has been far higher in Canada, doubling from 1990 to 2006. These data indicate that beyond the increase in number of publications shown in Figures 3 and 4, their quality relative to the rest of the world has also increased.
As another index of publication quality, the proportion of publications with at least one Canadian author among the 500 most highly cited child and youth health research papers between 1990 and 2008 increased from approximately 6% to more than 8% during this 18-year period.
Canadian reproductive and child health researchers have increased their relative (to CIHR overall) grant funding as well as the quantity and quality of their publications.
Figure 5: Mean number of citations of publications in child and youth health, Canada versus rest of the world, 1990-2006
Building capacity
As an institute focused on the health and development of the young, it was only natural for IHDCYH to take an active role in training new investigators in reproductive and child health and helping them get a good start in their research careers. As seen in Figure 1, training and salary awards in reproductive and child health research have continued to increase over the last 10 years when expressed as a percentage of overall CIHR expenditures in these categories. The figure shows this trend is similar for open and strategic awards.
The national grants program for new principal investigators (PIs), developed in collaboration with the SickKids Foundation (SKF), was IHDCYH’s first partnership external to CIHR. In total, IHDCYH and SKF have funded 98 of these grants for new PIs, thus providing a major boost to the early investigative careers of child and youth health researchers in Canada.
Shortly after IHDCYH’s scientific directorship transition in May 2003, Dr. Kramer and the Institute Advisory Board (IAB) made an important change in IHDCYH’s policy with respect to priority announcements in the Open Operating Grant Program. As of March 2003, IHDCYH has limited its $100,000 (maximum) one-year grants to start-up grants for new PIs, based on criteria similar to those in our new PI grants program with SKF. Since the inception of this program, IHDCYH has funded 50 of these start-up grants. In IHDCYH’s 2006 evaluation of the program, most new PIs reported that they obtained subsequent peer-reviewed funding from CIHR and/or other peer-reviewed funding agencies. They considered the initial start-up grant from IHDCYH to be a major factor in launching their investigative careers. In some cases, the grants prevented them from leaving research altogether.
In October 2003, Dr. Kramer, along with the other CIHR Institutes’ scientific directors, visited the U.S. National Institutes of Health and held bilateral meetings with senior scientific staff there. As a result of discussions with the National Institute of Child Health and Human Development (NICHD), collaborative, week-long Summer Institutes were developed in two strategically important areas of training for both Canada and the United States: reproductive and perinatal epidemiology and maternal-fetal pharmacology. Prior to this initiative, neither country had established training programs for graduate students or postdoctoral fellows in these areas.
These Summer Institutes have been remarkably successful. Every year since 2005, 20 participants have been selected for each institute from a highly competitive group of candidates from Canada, the U.S. and other countries. The week-long Summer Institutes combine lectures with small group discussions of research protocols, debates and other interactive formats to provide intense, stimulating and unique training experiences.
For the last several years, the Summer Institutes have been held simultaneously and have provided joint learning sessions and opportunities for informal social interaction between faculties and trainees. The Reproductive and Perinatal Epidemiology Summer Institute has spawned a new textbook co-authored by the Canadian and American faculty, which is due for publication in February 2011. It is important to note that these Summer Institutes resulted from the current scientific director’s approach to NICHD in 2003, rather than an approach from NICHD to IHDCYH.
The Summer Institute in Global Health Research is an initiative of the Canadian Coalition for Global Health Research, in collaboration with the Institute of Population and Public Health and several other CIHR Institutes, including IHDCYH. Its objectives are to nurture the next generation of global health researchers, facilitate North-South partnerships and promote action research. IHDCYH has participated in all of these Summer Institutes since 2005 and was a major organizer and funding partner in the sixth Summer Institute (held in Burkina Faso in 2009), which focused on maternal and child health research.
IHDCYH has invested heavily in the initial and renewal rounds of the Strategic Training Initiative in Health Research (STIHR) program. One IHDCYH-funded STIHR grant that deserves special mention is the Canadian Child Health Clinician Scientist Program, which was funded by IHDCYH and external partners. This unique program trains and supports new clinician-investigators in child and youth health research at the PhD, postdoctoral and new investigator career stages. The program provides support and multidisciplinary networking for practicing clinicians from diverse backgrounds, including medicine, nursing, psychology, physical and occupational therapy, and dietetics. Clinician scientists from a variety of clinical disciplines provide a rich mentoring network for this highly successful training program.
Finally, IHDCYH has held a series of career-development seminars in conjunction with regular annual scientific meetings of the Western and Eastern Perinatal Research Societies and the Canadian Fertility and Andrology Society. These seminars have been expanded to a full-day format, with a curriculum that includes grantsmanship; publication; ethics; knowledge translation (KT); mentorship; research supervision; how to balance investigative, clinical, teaching and university administrative activities; and work-life equilibrium. In 2006, the Institute held a stand-alone, two-day workshop on new PI career development jointly with the Institute of Genetics. The faculty for these seminars and workshops consists largely of current or former members of the IAB; most have been willing and eager to continue their participation in this activity. Evaluations of these seminars have been excellent and IHDCYH plans to offer them at least once or twice a year for the foreseeable future.
As an Institute focused on the health and development of the young, IHDCYH has succeeded in training, nurturing and supporting the careers of many new investigators in reproductive and child health.
Partnerships
Because of the plateau in the Institute’s strategic budget and our wish to increase impact on decision making,
IHDCYH has greatly increased its partnerships since the 2006 International Review report.
IHDCYH has partnered with all of the other CIHR Institutes, the Knowledge Translation Branch and the Ethics Office. External partners on IHDCYH-led initiatives have included the Heart and Stroke Foundation, Alberta Innovates - Health Solutions, Michael Smith Foundation for Medical Research, Fonds de la recherche en santé du Québec, Autism Speaks, AllerGen and Auto 21 Networks of Centres of Excellence, SickKids Foundation, National Child and Youth Health Coalition, Bloorview Children’s Hospital Foundation, Public Health Agency of Canada, First Nations and Inuit Health Branch, Health Canada, Ontario Neurotrauma Foundation, Alberta Centre for Child, Family and Community Research, Japanese Society for the Promotion of Science, National Natural Science Foundation of China, Chinese Ministry of Science and Technology, and Academy of Finland. IHDCYH-led strategic initiatives have benefited from $20.8 million in internal partnerships and have leveraged $25 million from external partners. IHDCYH has also contributed $1.7 million to initiatives led by other institutes, which have leveraged an additional $2.3 million from external partners.
Informing decision making
CIHR-funded research in reproductive and child health has not only created new knowledge (as revealed by the important publications cited below), but also facilitated the translation of that knowledge, with important impacts on decision making by clinicians, policy makers and the general public.
Clinical decision making
Based on the most recent data available, the number and total value of IHDCYH-affiliated randomized controlled trials (RCTs) in the area of reproductive and child health have been second only to those affiliated with the Institute of Circulatory and Respiratory Health since the inception of CIHR. Several of these RCTs have had important impacts on clinical decision making:
-
The Caffeine for Apnea of Prematurity trial (Dr. Barbara Schmidt, McMaster University) showed that not only did caffeine treatment of very preterm infants lead to a reduced risk of bronchopulmonary dysplasia (chronic lung disease of prematurity) during newborn hospitalization,Footnote 1 but also increased the likelihood of surviving without developmental disability by the end of the second year of life.Footnote 2 This trial received the inaugural Trial of the Year award from the Society for Clinical Trials and has led to routine use of caffeine therapy among very preterm infants, not only in Canada but internationally.
-
Dr. William Fraser of the Université de Montréal led an international, multi-centre RCT that demonstrated the ineffectiveness of amnioinfusion (saline infused into the amniotic fluid), which had been thought to reduce the risk of meconium aspiration syndrome by diluting the concentration of meconium in the inspired amniotic fluid.Footnote 3 The results led to the widespread discontinuation of this previously common clinical practice.
- The Multiple Courses of Antenatal Corticosteroids trial, led by Dr. Kellie Murphy of the University of Toronto, showed that multiple courses of antenatal steroids did not reduce mortality or morbidity from respiratory distress syndrome in preterm infants, and resulted in restricting fetal growth, including birth weight, length and head circumference.Footnote 4 These results led to a sharp reduction in the multiple courses of antenatal steroids previously used in Canada and internationally.
Informing public policy
CIHR-funded research has also had a major impact on public policy in the area of reproductive and child health:
-
Dr. Dave Ellemberg and his team from the Université de Montréal demonstrated that children and youth who sustain sports-related concussion injuries continued to have mild neurological deficits up to a year after the original injury.Footnote 5,Footnote 6 This research led to major changes in return-to-play policies, thus ensuring that Canadian children and youth can safely resume contact sports.
-
Dr. Stanley Zlotkin, a pediatric nutritionist from Toronto’s SickKids Hospital, has developed a small sachet called Sprinkles containing a one-day supply of powdered iron and other micronutrients, including zinc and vitamin A, that can be added to any semiliquid food, including porridge or yogurt, without changing its taste, colour or texture.Footnote 7 Sprinkles has reached four million at-risk children in more than 30 countries, and its distribution has been promoted by the World Health Organization (WHO), the World Food Program, and United Nations International Children’s Emergency Fund.
-
Dr. Joan Bottorff and her team from the University of British Columbia have focused on smoking and tobacco reduction in the context of women’s interactions and relationships with their partners.Footnote 8 This research has informed Health Canada guidelines that support pregnant women and new mothers to reduce and stop smoking. Information from one of the booklets developed from this project has also been adapted for use by the U.S. National Cancer Institute, Tobacco Control Branch in its website for pregnant smokers.
-
Dr. Michael Kramer, IHDCYH’s current scientific director, was asked by WHO to carry out a systematic review of evidence on the optimal duration of exclusive breastfeeding.Footnote 9 Part of that systematic review was based on his and his colleagues’ cluster-randomized trial of a breastfeeding promotion intervention in the Republic of Belarus. That trial and the subsequent systematic review led the World Health Assembly to revise its recommendation for the optimal duration of exclusive breastfeeding to six months (from four months).
- IHDCYH has also directly engaged members of the general public. The Institute has produced more than 50 communication activities over the last five years, including Café Scientifiques, journalist workshops, opinion articles and press releases. IHDCYH staff and affiliated researchers have been interviewed extensively by major media outlets across the country. In 2008-2009, the Institute’s scientific director was the top CIHR personality in the news, contributing to the organization’s visibility.
Impact on individual behaviours
CIHR-funded research in the area of reproductive and child health has also had a measurable impact on decision making involving behaviours by the general public, particularly in the area of injury prevention:
-
Dr. Anne Snowdon and her team at the University of Windsor developed an educational program, Bobby Shooster Rides Safely in His Booster, which included a children’s storybook, a growth chart to identify a correct safety seat for a child’s height and weight and a DVD to help parents correctly install safety seats. They demonstrated increases in knowledge and in the correct use of booster seats one year after the intervention.Footnote 10
- Dr. Brent Hagel and his colleagues at McGill University and the University of Calgary have published landmark researchFootnote 11 and systematic reviewsFootnote 12 demonstrating the efficacy of helmet use by skiers and snowboarders in protecting against head injury. These investigators have also shown that, despite conventional wisdom, helmets do not increase the risk of neck injury. These results have been widely publicized and likely have contributed to increased helmet use by skiers and snowboarders in Canada and abroad.
Health system impacts
Wait times for mental health services
Dr. Patrick McGrath’s CIHR-funded team from Dalhousie University developed a new program (Strongest Families) that provides greater access to mental health services for mothers and children for problems ranging from maternal postpartum depression to child anxiety and attention deficit/hyperactivity.Footnote 13 This research has markedly reduced wait times for children and families living in rural and remote areas of Nova Scotia and in one health district in Ontario. The families report excellent satisfaction with the improved access to convenient and effective interventions for their children, and administrators are pleased with the cost-effectiveness of these programs.
Screening for fetal alcohol spectrum disorder
Dr. Gideon Koren of Toronto’s SickKids Hospital and the University of Toronto has developed a new screening procedure for fetal alcohol spectrum disorder (FASD) in Canada based on measuring fatty acid ethyl esters found in meconium obtained in the first two or three days following birth.Footnote 14 This test has been adopted by the Public Health Agency of Canada as a screening tool for FASD. In partnership with the Canadian Association of Pediatric Health Centres, it is now being tested at various sites across the country.
Neonatal intensive care units
Dr. Shoo Lee (now at the University of Toronto) and his colleagues in the Canadian Neonatal Network carried out a cluster-randomized trial of two interventions, one to reduce the risk of neonatal sepsis, the other to reduce the risk of bronchopulmonary dysplasia (chronic lung disease of prematurity), in 12 neonatal intensive care units (NICUs) across Canada.Footnote 15 The trial was based on an innovative, network-wide approach to designing and implementing the two experimental interventions. The results have led to major changes in clinical care in NICUs across the country.
Economic impacts
The above-mentioned trial from the Canadian Neonatal Network has decreased average NICU length of stay by two days, translating into potential savings of $40 million per year. The network has also compared outcomes for retinopathy of prematurity (ROP) at the various sites participating in the Network with widely differing practices for screening.Footnote 16 Their results should reduce by 50% the number of preterm infants routinely screened for ROP and thereby reduce health care costs by more than $1 million per year in Network NICUs.
The Neonatal Network has also patented a new clinical measurement tool called the SNAP II, an improvement over the original SNAP (score for neonatal acute physiology).Footnote 17 The new tool is becoming an international standard for assessing severity of neonatal illness and comparing outcomes from hospital to hospital. SNAP II has been licensed to insurance companies and has already had an impact on insurance reimbursement based on illness severity.
Dr. Anne Snowdon and her colleagues at the University of Windsor not only succeeded in improving parents’ use of car booster seats (see above), but also worked with Magna International to design and manufacture the Clek, an improved booster seat that is more acceptable to children than conventional seats and thus more likely to be used. The Clek, launched in Canada in 2006 and in the U.S. in 2007, has won several national and international awards.
CIHR and IHDCYH have responded to their KT mandate and the recommendations of the 2006 International Review by funding and/or facilitating research that has impacted on decision making by clinicians, policy makers and the general public, on the health system and on the Canadian economy.
Transformative impacts
Our research community
The increase in breadth, depth and cohesion of the Canadian reproductive and child health research community would not have been achieved without IHDCYH’s involvement. Primary among these transformative impacts is multidisciplinary collaboration. Although Canada had strong individuals and small collaborative teams in these research areas before IHDCYH, teams tended to work within, rather than across, disciplines. IHDCYH’s team-grant requests for applications (RFAs), which required collaboration among investigators from at least three of CIHR’s four research themes, encouraged such multidisciplinary collaboration. Many IHDCYHfunded teams have continued their research beyond the RFAs that led to their creation, including receipt of other team grants, open operating grants and new STIHR programs.
IHDCYH has also helped unite the reproductive and child health communities. Although obstetric and neonatal researchers collaborated prior to IHDCYH, the degree of collaboration across reproductive and child health research has increased with IHDCYH’s and CIHR’s funding of cohort studies that begin during pregnancy and continue with long-term child health follow-up. The Maternal, Infant, Child and Youth Research Network (MICYRN) was developed under IHDCYH’s encouragement of the reproductive and child health research communities to submit a joint application to CIHR’s Clinical Research Initiative (CRI). Although the CRI application was not funded, MICYRN has received funding from other sources and has continued to be a unifying force for maternal and child health research in Canada. Most recently, IHDCYH and MICYRN partnered to develop an inventory of pregnancy/birth cohort studies,Footnote 18 which will be regularly updated and enable investigators to increase their collaboration throughout the life course.
Health and environment
In the absence of an institute on environmental health, IHDCYH has championed research in this area at CIHR. With internal partnering by the Institute of Genetics, the Institute of Infection and Immunity, the Institute of Gender and Health, the Institute of Aboriginal Peoples’ Health and the Institute of Circulatory and Respiratory Health, and external partnering by the AllerGen Network of Centres of Excellence, Health Canada, and the Canada Mortgage and Housing Corporation, IHDCYH launched and co-funded a large (more than $2 million per year over six years), multi-centre pregnancy/birth cohort study of the effect of indoor air quality on the development of childhood asthma and allergy. This study should make an important contribution to knowledge about the etiologic role of indoor pollutants and moulds that will inform future Canadian regulations for home construction, ventilation and humidification.
As described in an earlier section, IHDCYH partnered with Health Canada to fund two large multidisciplinary teams to investigate the potential adverse effects of major endocrine-disrupting environmental contaminants (one team on phthalates, the other on brominated flame retardants) on key reproductive health outcomes. The resulting research will inform Health Canada’s regulatory policy for these important environmental contaminants.
Injury research
IHDCYH championed the Strategic Teams in Applied Injury Research initiative, a multi-institute, multi-partnered RFA focused on etiologic, preventive and health services research to reduce the mortality and morbidity of injury in Canada. Injury research is a high priority for the current federal government and the teams funded by this initiative were recently the subject of a major public announcement by the Minister of Health. Intentional and unintentional injury is one of IHDCYH’s four research priority areas, and this initiative would not have been launched without IHDCYH’s leadership.
Ethics
A major challenge of child and youth research is to ensure that advances are achieved in a way that maximizes benefits, minimizes potential harm and respects parental authority and the developing autonomy of minors. Most of the ethical norms governing research involving human subjects do not take a clear position on child and youth research. They usually indicate in a general manner that children and adolescents should be included in \research without providing further guidance. The increasing demand to include children and adolescents in research areas such as genomics, randomized trials of new drug therapies and cohort (longitudinal) studies requires new and updated ethical guidance that keeps pace with the possibilities of emerging technology.
In collaboration with CIHR’s Ethics Office, the Centre of Genomics and Policy (McGill University), the National Council on Ethics in Human Research, the Public Health Agency of Canada, Health Canada and MICYRN, IHDCYH has funded and logistically supported the development of a document that proposes best practices for research involving children and youth. With an extensive inventory of current international thinking and protocols, this landmark document addresses the particular ethical and legal issues raised by current and emerging trends in child and youth research, and proposes practical solutions for researchers and research ethics boards.Footnote 19
International collaboration
IHDCYH has championed a number of collaborative research and/or research training programs with funding agencies in other countries:
-
China - CIHR’s collaborative grants program with the National Natural Science Foundation of China, in which IHDCYH is a major internal partner, is limited to theme 1 (basic science) research. IHDCYH wished to expand Sino-Canadian collaborative research in reproductive and child health to other research themes. After consultations with medical faculties, reproductive and child health researchers and federal ministries in China, IHDCYH spearheaded a new collaborative grants program with the Ministry of Science and Technology. In 2010, this resulted in six teams co-funded by six CIHR Institutes, each to a total of $1 million over three years, with a second competition planned afterward. Most of these team grants also involve multiple disciplines, including researchers from basic science, clinical and population health research.
-
India - A CIHR delegation to India in the fall of 2005 resulted in the signing of a memorandum of understanding (MOU) for collaborative research between CIHR and the Indian Council of Medical Research (ICMR). Although IHDCYH’s scientific director was not part of the original delegation, IHDCYH was the first institute to follow through with the MOU. After a successful workshop in New Delhi in January 2009, an RFA was launched for Indo-Canadian multidisciplinary teams to investigate the causes and prevention of child obesity. The Institute of Nutrition, Metabolism and Diabetes subsequently agreed to co-fund one of these teams. IHDCYH is planning further collaboration with ICMR and with the Industrial Credit and Investment Corporation of India’s Centre for Child Health and Nutrition to develop a strategic initiative in perinatal health research.
-
WHO - IHDCYH has also developed a fruitful collaboration with the Department of Reproductive Health and Research (RHR) at WHO. This collaboration resulted in an invitation for Canada to be the only developed country to participate in WHO’s Global Survey of Maternal and Infant Health, the initial focus of which was the causes and consequences of the large variation in caesarean delivery rates within and between countries. IHDCYH awarded a three-year team grant under this RFA based on a common protocol and data collection strategy developed by WHO. Data collection for this survey has been completed and results will be available soon.
-
WHO - In October 2009, IHDCYH facilitated and co-funded (with RHR and the National Institutes of Health [NIH]) an important workshop in Ottawa on scaling up effective reproductive and perinatal health interventions in low- and middle-income countries. The workshop included NIH’s Fogarty Center, WHO and a group of investigators from Latin America, Europe, Canada and the United States. Canada’s internationally recognized expertise in the methodology of cluster-randomized trials and the scaling-up of interventions were key to the success of this workshop. The result was a protocol (now referred to as the Ottawa Protocol) for a cluster-randomized trial to evaluate scaling-up strategies for administering magnesium sulfate to reduce maternal mortality in women with eclampsia and, secondarily, a possible future trial of calcium supplementation in countries or regions with low dietary calcium intakes.
- International Collaborative Group in Maternal Mortality and Severe Morbidity - In November 2008, IHDCYH organized, hosted and co-funded (with the U.S. Centers for Disease Control and Prevention) an international workshop of investigators from Canada, the U.S., UK, France, Belgium and Australia to review the increase in postpartum hemorrhage recently reported in several developed countries. The workshop led to a data pooling effort and an important publication co-authored by the workshop participants.Footnote 20 A follow-up meeting on amniotic fluid embolism (another major cause of maternal mortality and severe morbidity in developed countries) was hosted in July 2010 by the UK’s National Perinatal Epidemiology Unit, with work now under way for a pooled analysis and joint publication. This successful international working group plans to continue its collaboration; its next focus will be maternal mortality from cardiac and cerebrovascular disease.
IHDCYH has transformed Canada’s reproductive and child health research landscape and increased its international stature in this domain.
Going Forward
Alignment with Roadmap
IHDCYH has already aligned its strategic priorities to cohere with those of CIHR’s Roadmap. Our broad mandate is both a challenge and an opportunity, because it cuts across all four CIHR research themes. Our focus on development and life-course transitions will ensure that future investments remain strategic by helping us avoid doing too little in too many areas.
Well before the release of Roadmap in the fall of 2009, IHDCYH knew of Canada’s weakness in the area of reproductive and child health services and policy research (HSPR) and had instituted steps to correct that weakness. With greater emphasis on health services in Roadmap, these attempts have been redoubled over the last year, including appointing new members to IHDCYH’s Institute Advisory Board (IAB) who have HSPR expertise, and planning requests for applications (RFAs) in the areas of capacity building in HSPR, access to mental health services and primary care. The Institute of Health Services and Policy Research (IHSPR) has helped us prioritize potential solutions to improve support for this important area of health research in Canada.
Another of Roadmap’s strategic priorities is reducing health disparities for Aboriginal and other vulnerable populations. Since IHDCYH’s beginnings, we have partnered with other institutes (particularly the Institute of Gender and Health) to fund RFAs in health disparities involving mothers and children. Going forward, IHDCYH sees a need to work even more closely with the Institute of Aboriginal Peoples’ Health and Health Canada’s First Nations and Inuit Health Branch toward developing and testing interventions that will improve the health and health care of Aboriginal mothers and children in Canada.
In alignment with Roadmap’s strategic priority on chronic disease and mental illness, HDCYH will continue to devote much of its strategic funding to research in the area of mental health and addiction of mothers, children and youth. Moreover, the Institute plans to continue funding research in the early origins of obesity, the causes and prevention of asthma, improving quality of life in children with disabilities and the developmental origins of adult chronic disease.
Leadership
One challenge facing IHDCYH over the next two years will be the transition to a new scientific director and, presumably, a new location. Although no radical changes in direction are anticipated, the arrival of new staff will add fresh vision and energy to reproductive and child health research in Canada as the Institute faces current and future challenges. Elisabeth Fowler, IHDCYH’s recently appointed, Ottawa-based assistant director, will have developed sufficient institutional memory to ensure a smooth transition for the new Institute.
A recent emphasis of the current leadership is the need for increased interaction with the provinces and territories, particularly in the area of HSPR. The success of future RFAs will depend on such collaboration, not only in financial terms, but also to ensure that questions addressed by future RFAs in HSPR are priorities for the jurisdictions responsible for health services and programs. Increased interaction with the provinces and territories will also profit from new tools developed by IHSPR and the KT branch, such as Evidence on Tap and Best Brains, which will increase IHDCYH researchers’ impact on decision making.
New developments and emerging issues
Although it is difficult to foresee the impact of new scientific discoveries and health care challenges on IHDCYH’s long-term strategic priorities, several areas have already emerged as important. Likely, the developmental origins of health and disease will continue to benefit from new scientific discoveries and new opportunities for strategic research. Developmental neuroscience has already received considerable IHDCYH funding. In future, emerging scientific discoveries about the prenatal and early postnatal neural circuits that develop in response to the physical environment, social environment and nutrition ensure that this will be an increasingly important area for investment. Finally, new legislation in Quebec funding single-embryo transfer for infertile couples will create unique opportunities for research and knowledge translation (KT) in assisted reproductive technologies.
More generally, research that explores the interactions between the genome and all aspects of the environment via epigenetic or other mechanisms will continue to create new opportunities and priorities for strategic research investment. CIHR and IHDCYH should continue to advocate for a large pregnancy/birth cohort study to assess the effects of exposure to environmental contaminants on birth outcomes, sexual development and neurobehavioural function, since such effects are extremely difficult to investigate via conventional (five-year maximum) CIHR operating grants.
In the past, IHDCYH launched two theme 3-oriented RFAs: a team grant to fund Canada’s participation in the World Health Organization global survey of the determinants and consequences of variations in caesarean delivery rates, and an RFA on indicators of health and of access to and quality of health care services for children and youth. Yet it was clear that HSPR would need increased attention in the years to come, particularly in view of an upcoming re-negotiation of the health accord between the federal government and the provinces and the continued strain over funding in Canada’s health care system.
In early 2011, IHDCYH will relaunch an RFA to support the linkage and secondary analysis of population health and health services databases. We have also held consensus workshops to develop RFAs in the areas of capacity building in reproductive and child HSPR and access to mental health services, and a satellite workshop at the Primary Care Summit led by IHSPR. Improvement of primary health care for pregnant women, children and youth in Canada will require the development and testing of new models for delivery and access to primary health care services, such as patient-centered team care. The Institute plans to invest heavily in these theme 3 areas through targeted RFAs in partnership with provincial governments, the Mental Health Commission of Canada, IHSPR and other CIHR Institutes.
Lessons learned
We are confident that some of the lessons IHDCYH has learned in its first 10 years will continue to guide the leadership. One of IHDCYH’s earliest and most successful efforts was its emphasis on multidisciplinary, multi-theme research collaboration. Such collaboration was rare under the Medical Research Council, as individual researchers had little motivation, or even opportunity, to collaborate with scientists from other disciplines and themes. While it is too early to tell whether such collaboration will have a greater impact on health and health care, this strategic direction has already been lauded by researchers from across the disciplines and themes as intellectually stimulating, innovative and creative and has led to new knowledge and new applications of that knowledge.
A second important lesson is that true knowledge translation benefits from, and may even require, integrated KT, rather than end-of-grant KT. It is difficult and often futile to attempt to apply new knowledge when that knowledge was created without the participation of decision makers (be they the general public, health care providers or policy makers) in posing the research questions, choosing the research methods and analyzing and interpreting the resulting data. IHDCYH and its institute partners agree that involving such decision makers at the very earliest stages of RFA development is essential to increase the likelihood that research findings actually influence decisions. When decision makers co-fund these initiatives, their financial stake increases the likelihood that the research will succeed and findings will be applied. Increasingly, such decision makers work outside the health sector (e.g., education, social services and justice). This is particularly important for an institute such as IHDCYH, which has few opportunities for commercial partnerships. Pharmaceutical companies, for example, tend to avoid developing and testing new drugs for pregnant women and children for fear of unforeseen adverse effects and costly litigation.
A third important lesson has been the importance of listening to and supporting IHDCYH’s research community. It will be important for IHDCYH’s future leadership to build on recent accomplishments in cementing the reproductive and child health research community in Canada. This cohesion has been achieved as a result of funding investigator-initiated workshops, travel awards for trainees, lectureships, skills update awards and career development seminars. Perhaps more useful have been IHDCYH’s interactions with the reproductive and child health research communities at academic institutions across the country during the IAB’s biannual face-to-face meetings. In conjunction with those IAB meetings, IHDCYH collaborates with local researchers to organize half-day workshops, debates, scientific presentations and informal social gatherings to ensure two-way communication between these local research communities and the IHDCYH leadership.
Through our collaborative grants program with the SickKids Foundation, priority announcements in CIHR’s Open Operating Grants Program, Summer Institutes and career-development workshops, IHDCYH is recognized across the country for its efforts to support trainees and new principal investigators in reproductive and child health. Finally, IHDCYH has strengthened its national profile by its presence at, and contribution to, Canadian scientific and clinical meetings in the areas of the Institute’s mandate. It has done this through activities such as judging poster competitions, awarding prizes and offering KT and scientific seminars on specific topics.
All these activities have contributed to IHDCYH’s recent success at building a strong and cohesive research community in reproductive and child heath. Continuing such support will help us achieve our mission to improve the health and health care of mothers, children and youth in Canada and beyond.
IHDCYH has helped build a strong, cohesive research community poised to face the reproductive and child health challenges of the 21st century.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
IHDCYH specific
| ARC | average of relative citations |
| CRI | Clinical Research Initiative |
| FASD | fetal alcohol spectrum disorder |
| HSPR | health services and policy research |
| IAB | Institute Advisory Board |
| ICMR | Indian Council of Medical Research |
| KT | knowledge translation |
| MICYRN | Maternal, Infant, Child and Youth Research Network |
| MOU | memorandum of understanding |
| NICHD | National Institute of Child Health and Human Development |
| NICU | neonatal intensive care unit |
| NIH | National Institutes of Health |
| PI | principal investigator |
| RCT | randomized controlled trial |
| RFA | request for applications |
| RHR | Reproductive Health and Research |
| ROP | retinopathy of prematurity |
| SI | specialization index |
| SKF | SickKids Foundation |
| SNAP | score for neonatal acute physiology |
| STIHR | Strategic Training Initiative in Health Research |
| WHO | World Health Organization |
- Date modified: