Internal Assessment for 2011 International Review - CIHR Institute of Cancer Research
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures
- Figure 1: CIHR expenditures and number of grants relevant to ICR mandate, by fiscal year
- Figure 2: Percentage of total CIHR expenditures related to ICR mandate areas over time
- Figure 3: Specialization index and average of relative citations (ARC) for top 10 countries publishing in PEOLC, 2000–2008
- Figure 4: ICR investment in cancer research by theme, 2000–2010
- Figure 5: Co-publications among members of PEOLC New Emerging Teams
Mandate and Context
Mandate and mission
Created in 2000 as one of the 13 institutes of the Canadian Institutes of Health Research (CIHR), the Institute of Cancer Research (ICR) has a mandate to support research that reduces the burden of cancer on individuals and families through prevention strategies, screening, diagnosis, effective treatments, psychosocial support systems and palliation. The ICR mandate transcends disciplines and encompasses all four health research themes: biomedical; clinical; health systems and services; and social, cultural and environmental factors that affect the health of populations. ICR's mission is to foster research based on internationally accepted standards of excellence that bear on preventing and treating cancer, and improving the health and quality of life of cancer patients and survivors.
Structure and operations
The Institute is supported by a small staff based at ICR offices at McGill University in Montreal, and also at CIHR headquarters in Ottawa. ICR is guided in its activities by an Institute Advisory Board (IAB). The IAB is comprised of leading researchers, partners and research users drawn from the full spectrum of the cancer control field – from lay persons and survivors to molecular geneticists, epidemiologists, clinicians and an ethics designate. The IAB generally meets three times a year. In 2008, ICR underwent transition and Dr. Morag Park assumed the leadership from inaugural Scientific Director Dr. Philip Branton.
Additional funds managed by ICR: the Cancer Stem Cell Consortium
In 2007, several of Canada's leading research-funding agencies with a shared interest in cancer stem cells formed the Cancer Stem Cell Consortium (CSCC). CSCC was created to accelerate the translation of cancer stem cell research into clinical applications through the support of large-scale cancer stem-cell research programs and related platforms.Footnote 1 Current members of the CSCC include the Canada Foundation for Innovation, Genome Canada, the Canadian Institutes of Health Research, the Ontario Institute for Cancer Research and the Stem Cell Network –one of the Networks of Centres of Excellence. CIHR has committed $30 million over five years, including $5 million from ICR, to support the activities of CSCC. The CIHR investment in CSCC is managed by ICR.
Recommendations from the 2006 CIHR International Review
The 2006 International Review commended ICR on its partnership and community-building activities and the Institute's ability to bring about organizational change. The Institute also received positive feedback on its delivery on the CIHR mandate in the area of knowledge creation. Recommendations for improvement included an increased emphasis on knowledge translation (KT) and communications activities, especially with individual researchers. It was also suggested that the Institute review its efforts in support of ethics and establish effective performance targets.
ICR's response to the 2006 review
Knowledge translation
In the area of knowledge translation, ICR has developed several initiatives with a focus on integrated KT and frequently takes advantage of the suite of open competitions managed by the CIHR KT branch to support KT activities in the cancer community. In addition to providing support for meetings, planning and knowledge-dissemination activities, the Institute now offers travel awards that enable students and postdoctoral fellows to attend national and international workshops and symposia. This encourages career development and knowledge dissemination.
Communications and community engagement
To improve communications with the cancer-research community, ICR now distributes regular newsletters with information on ICR activities, cancer-related events and funding opportunities. The Institute has also organized three Café Scientifiques across Canada in London, Vancouver and Quebec City, and is planning a fourth in Montreal in 2011. These events are well attended by the local research community and the general public. ICR staff attends and presents at many cancer-related meetings, workshops and symposia each year, often with the CIHR information booth, to provide a venue for discussion with the research community. The Institute recently launched the Publication Prize Program to recognize excellent research performed by students and postdoctoral fellows and to establish linkages with individuals. ICR generates prominent coverage in the media, and is often among the top three institutes most quoted each quarter. Numerous ICR-related initiatives such as cancer stem cells and medical imaging have generated considerable media interest.
Ethics
The Institute is fully supportive of the movement towards central research ethics board review and has actively supported CIHR's efforts to establish a national centre for the scientific review of multi-centre cancer clinical trials. Several ICR-supported collaborative initiatives, such as cancer stem cell research funding though the Cancer Stem Cell Consortium (CSCC), a recently launched program on rare diseases led by the CIHR Institute of Genetics and a joint Genome Canada initiative on childhood diseases include a strong focus on ethics and a specific request for applications in ethics.
The Institute responded to mid-term review by increasing its knowledge translation, communications, community-engagement and ethics activities.
The Canadian context – evolution of the cancer research landscape
Prior to the creation of CIHR, Canadian cancer research was funded primarily by the Medical Research Council, a few provincial cancer agencies and a handful of cancer charities, the largest of which was the National Cancer Institute of Canada. In recent years, new organizations such as the Ontario Institute of Cancer Research and the Terry Fox Research Institute have entered the field. A recent estimate shows that Canadian research investment in peer reviewed grants was more than $400 million in 2007, CIHR remaining the largest single investor and contributing about 30% of the total funding.Footnote 2 With a current Institute strategic initiative budget of $8.5 million per year – less than 3% of the total estimated annual investment in cancer research – the challenge for ICR has not been how to build a community but how to identify a niche within the existing community that would enable the Institute to have an impact on cancer control. The Institute has addressed this challenge through a series of highly targeted strategic initiatives.
The Institute began as a small player in an already well established and well funded Canadian cancer research community.
A growth in CIHR cancer research funding
The CIHR investment in open and strategic cancer research increased consistently from 2000–2001 to 2008–2009, followed by a period of reduced growth in recent years (Figure 1).
Figure 1: CIHR expenditures and number of grants relevant to ICR mandate, by fiscal year
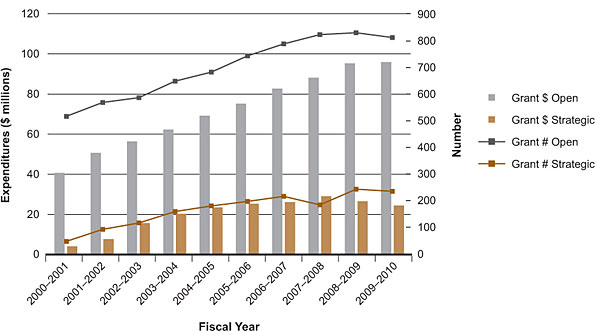
Data in Figures 1 and 2 are based on a keyword search of the CIHR funding database and validated through a subjective process. Projects may have multiple institute affiliations.
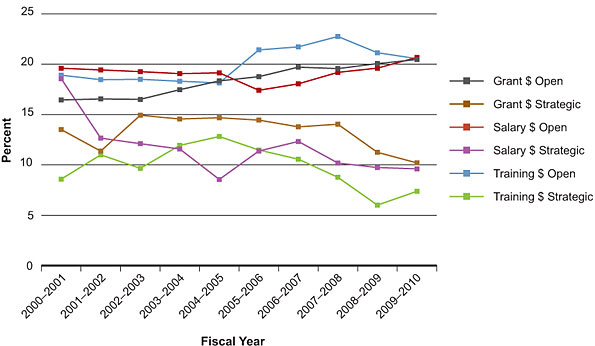
Figure 2 shows the percentage of CIHR expenditures supporting cancer research through grant, salary and training awards. The vast majority of cancer research funding comes from the CIHR Open Grants competitions. In this area, growth in the cancer community has either kept pace or exceeded the growth in overall CIHR funding, with the percentage of cancer-related CIHR funding in this category increasing from 16% ($41 million) in 2000–2001 to 20% ($96 million) in 2009–2010. For salary awards, the proportion invested through open competitions has remained consistently higher than that invested through strategic funds (21% and 10% respectively for 2009–2010). Variation over time reflects changes in overall CIHR programs and funding patterns as well as strategic investment.
Figure 2: Percentage of total CIHR expenditures related to ICR mandate areas over time
Institute Priorities
Training the next generation of cancer researchers
An overarching priority for ICR has been training; the Institute supported all three rounds of the CIHR Strategic Training Initiative in Health Research (STIHR) program. In addition, ICR partnered with the Institute of Genetics to host two young investigator meetings (2004, 2006), and with the National Cancer Institute of Canada (NCIC) to co-host the 2005 national meeting for cancer research trainees. Training is a major component of ICR strategic initiatives as evidenced by the Palliative and End-of-Life Care Initiative. Training occurs through the creation and support of emerging teams that recruit and mentor students and postdoctoral fellows.
The first strategic plan: a priority-setting exercise
The Institute's first priority-setting exercise began in 2001 with a large working group meeting organized by ICR, NCIC, the Canadian Association of Provincial Cancer Agencies (CAPCA) and Health Canada and involving cancer researchers from all health research themes, lay persons, survivors and potential partners. This meeting led to a web-based Delphi process to further refine priorities and seek input from the broader community. The result was the identification of 24 priority areas, from which six were selected by the Institute Advisory Board (IAB) and representatives from NCIC, CAPCA and Health Canada. In order of votes received, the six priorities were: palliative and end-of-life care; molecular profiling of tumours; clinical trials, early detection of cancer; risk behaviour and prevention; and molecular and functional imaging. A multidisciplinary working group was created for each priority and chaired or co-chaired by an IAB member. The groups were tasked with developing strategic research initiatives to address each priority area. In 2004, an additional research priority, access to quality cancer care, was added in response to a new government priority in this area.
The second strategic plan: refocusing priorities
In 2008, in preparation for Institute transition, ICR held a consultation workshop with current and past IAB members, representatives of the major cancer funding agencies and the decision and policy-making communities. Participants reviewed the original ICR priorities and developed a set of criteria for selecting new, more focused priorities. To integrate these priorities into the overall cancer funding landscape, ICR assumed a key role in a national consultation, spearheaded by the Canadian Cancer Research Alliance, an alliance of Canadian cancer research funders. The outcome was the development of a pan-Canadian cancer research strategy.Footnote 3 This national strategy will provide a framework to guide cancer research investment in Canada, highlight gaps and opportunities for new collaborations, and provide a vision for cancer research achievements for the next five years.
ICR played a leadership role in the development of the first pan-Canadian cancer research strategy.
Evolution of research priorities
ICR's second strategic plan (2010–2015) identifies four broad strategic priority areas:
- Cancer prevention: lifestyle, environment and cancer
- Diagnosis and guided therapy: towards personalized medicine
- Cancer-initiating cells
- Survivorship
These priorities reflect advances in cancer research since 2000, such as increased understanding of the role of cancer stem-like cells and the tumour microenvironment in tumour initiation and progression, and also the emergence of new fields of study and new technologies that have made the prospect of moving towards personalized medicine a reality. The priorities also recognize a new reality – the increasing success of new treatments and therapeutics in prolonging the lifespan or effecting cure – and the health issues experienced by a growing cohort of cancer survivors. ICR's new strategic priorities align well with the CIHR strategic plan for 2009–2014, called Health Research Roadmap: Creating innovative research for better health and health care. ICR aligns particularly with priority areas 1, Enhance patient-oriented care and improve clinical results through scientific and technological innovations; and 2, Promote health and reduce the burden of chronic disease and mental illness.
Key Initiatives
Over the last 10 years, the Institute has developed initiatives to address all its priorities. Examples include the ongoing support of a national tumour bank network (CTRNet) that provides a valuable infrastructure for the cancer research community, support for cancer clinical trials through a partnership with the National Cancer Institute of Canada and sustained support for the Tobacco Control Research Initiative, a multi-organizational partnership created to address tobacco-related research issues. The initiatives described below highlight the Institute's achievements in transforming underserved research areas and illustrate the flexibility of the Institute model in facilitating collaborations and responding to health crises. The lessons learned from these initiatives will serve ICR well as it plans future programs.
Initiative 1: Palliative and end-of-life care
The research challenge
The demand for high quality palliative and end-of-life care (PEOLC) is increasing as baby boomers enter old age. Advances in modern medicine are prolonging the lifespan but often with the result that the elderly are now living with a variety of chronic, life-limiting diseases. Towards the end of life, many people who could benefit from PEOLC do not receive it.Footnote 4 All too often it is left to patients, their families and friends and a loosely knit community of volunteer organizations to deal with physical, psychological, spiritual and ethical choices. It was this reality that led to the identification of PEOLC as ICR's number one research priority and its acceptance by the larger cancer research community.
In 2003, Canadian palliative care research was defined by a small, dedicated but under-developed research community, which was struggling to gain recognition for the field as an independent health discipline. Palliative care research tends to be highly applied, practice oriented and mostly undertaken by health care providers. This presents many methodological, logistical and ethical challenges. PEOLC research requires study designs that address the reality and special needs of an extremely vulnerable population.
The scope of the PEOLC initiative
ICR realized from the outset that PEOLC, although historically associated with cancer, was equally relevant in many other health disciplines such as cardiology, respiratory medicine, critical care, nephrology, pediatrics and neurology. Therefore, ICR engaged other research communities as it developed the initiative. ICR also recognized the importance of partnerships in leveraging the Institute's funding envelope for PEOLC. Following a series of planning meetings and partner negotiations, ICR launched the PEOLC initiative in 2003. Prior to this, the Institute primed the community by funding a palliative care training program in the CIHR Strategic Training Initiative in Health Research (STIHR) in partnership with the National Cancer Institute of Canada, and by co-funding a palliative care New Emerging Team Grant in partnership with the CIHR Institute of Aging. By the time the PEOLC initiative was launched, ICR had engaged 16 partners to support Canadian PEOLC research, including seven other CIHR institutes, the CIHR Knowledge Translation Branch, four voluntary sector organizations, three provincial cancer agencies and Health Canada.Footnote 4
The results of the PEOLC initiative
By 2004, the PEOLC initiative had funded 19 pilot projects, one career transition award, a training program and 10 New Emerging Teams, for a total investment of $16.8 million over six years by ICR and partners.
In 2004, the ICR-led PEOLC initiative was the world's biggest single initiative in PEOLC and represented an achievement that would have been unlikely prior to the creation of CIHR and the institute model.
The Initiative gained the attention of the National Cancer Research Institute (NCRI) in the United Kingdom (UK), which had identified PEOLC as a priority area. ICR engaged with NCRI to organize a UK workshop, in collaboration with the United States (U.S.) National Cancer Institute, for Canadian, UK and U.S. PEOLC researchers. The workshop reportFootnote 5 identifies many common challenges and opportunities for international partnerships, some of which have been realized by individual researchers. The PEOLC initiative is frequently presented at national and international meetings as a model for PEOLC research.Footnote 6
Preparing for future sustainability
To sustain capacity and enhance support for PEOLC research overall, CIHR, at the request of ICR, created a new, dedicated and permanent operating grant peer review committee to better serve the needs of the PEOLC community.
Initiative 2: Access to quality cancer care
This initiative further illustrates ICR's capacity to build partnerships and engage the anticipated end users of research outcomes in the research process. It also demonstrates the Institute's ability to respond to emerging research gaps.
The research challenge
The Access to Quality Cancer Care (AQCC) initiative was developed primarily to build capacity in the cancer health services research field. Despite an increase in overall health services research spurred by the CIHR Institute of Health Services and Policy Research, capacity was not increasing in the cancer domain. The initiative built on CIHR's response to the federal government's identification of timely access to high quality health care as a major priority in 2004. This announcement was followed by the 2005 launch of the CIHR initiative Towards Canadian Benchmarks for Health Services Wait Times – Evidence, Application and Research Priorities. ICR partnered on this rapid-response initiative, funding four cancer-related projects tasked with establishing benchmarks for wait times in cancer diagnosis and treatment. The AQCC initiative was developed to expand ICR's response beyond wait times to the broader issues related to access to cancer care.
The scope of the AQCC initiative
From the outset, ICR realized the importance of engaging health system managers and policy makers in the development of this initiative and particularly the provinces, as the deliverers of health care, through the provincial cancer agencies. A June 2005 consultation workshop attended by representatives of all the relevant communities led to recommendations that formed the basis of a request for applications (RFA). The AQCC initiative was launched in 2005 with 13 partners, including eight provincial cancer agencies.
The results of the AQCC initiative
This initiative resulted in the 2007 funding of seven research teams in five provinces for an investment by ICR and partners of more than $10 million. Three of the teams were co-funded by their respective provincial cancer agencies to facilitate the translation of their research outcomes directly into health care policy. In 2009, ICR organized a networking and knowledge translation (KT) workshop for the funded teams. Teams were encouraged to engage with policy makers in order to strengthen their KT strategies and think about the sustainability of their projects beyond the five years of their grants.
ICR built key partnerships and engaged the anticipated end users in the research process to improve access to quality cancer care.
Colorectal cancer screening
The AQCC initiative focused not only on equitable access to cancer care for all Canadians, but also on the quality of that care. One research question addressed under the AQCC initiative was how best to deliver a population-based colorectal screening program. Canada has one of the highest incidences of colorectal cancer in the world.Footnote 7 Regular screening can diagnose the disease at an early stage and is proven to reduce mortality from colon cancer.Footnote 8 It can also prevent the disease through detection of precancerous polyps, which can be easily removed. However, equitable access to colorectal cancer screening programs poses many challenges, including the development of specific, sensitive and user-friendly screening tests and the implementation of a national screening program. ICR has addressed colorectal cancer screening through several interconnected programs, including one-year operating grants, one-year pilot projects and five-year Emerging Team Grants for a total investment of $6 million. Early research outcomes from some of these programs will be described in the Outputs and Outcomes section of this report.
Initiative 3: Medical imaging
This initiative highlights a further strength of the institute model – the capacity to respond rapidly to a health crisis. Molecular and functional imaging was one of ICR's original priorities and, based on the recommendations of the working group, the Novel Technology Applications in Health Research initiative was launched in 2003. This initiative addressed the need to integrate emerging imaging technologies from fields outside the life sciences with biomedical and clinical research methodologies. Although a modest initiative that funded four projects for two years, the outcomes have been significant and ICR identified medical imaging as a continuing priority moving forward.
Responding to a health crisis
In the wake of repeated closures of the aging nuclear reactor at Chalk River, ICR took the lead in coordinating the CIHR response to the resulting isotope shortage that caused critical challenges in medical imaging. ICR engaged five other CIHR institutes and the Natural Sciences and Engineering Research Council (NSERC) to launch the Operating grant: Alternative Radiopharmaceuticals for Medical Imaging initiative in June 2009.
ICR took the lead in coordinating a research response to an isotope shortage that was causing a critical situation in the health care system.
Collectively, the institutes and NSERC committed $6 million over two years to support this initiative. The objective was to speed the development of replacements for the 99mTc-labeled, reactor-produced radiopharmaceuticals and support research on alternative means of 99mTc production that do not require the use of a nuclear reactor. Funding was provided to support clinical trials applications and small-scale clinical validation studies that would compare novel radiolabeled probes with those in current practice within two years or less.
To promote innovation and networking, no funding cap was imposed on individual grants. This led to the funding in January 2010 of seven projects including an ambitious multicentre study led by Drs. François Bénard and Tom Ruth, to develop methods for the production of technetium radioisotopes using cyclotrons instead of nuclear reactors. Several institutes, including ICR, provided funding for highly ranked projects even though they were not strictly within individual institute mandates. This is a stellar example of the collaborative institute model in action.
Engaging the broader imaging community
In October 2009, ICR and NSERC organized a joint workshop on medical imaging to unite researchers from the life and physical sciences and forge linkages between the medical disciplines that rely on medical imaging for patient management. The workshop's recommendations included the creation of a national imaging clinical trials network.Footnote 9 In Budget 2010, the federal government announced $10 million over two years for CIHR to establish this network.Footnote 10 In June 2010, ICR, together with the CIHR Strategy for Patient Oriented Research, launched an RFA for a medical imaging clinical trials network. ICR and the Institute of Circulatory and Respiratory Health have worked closely with their respective imaging communities in recent years, fostering interactions between these previously unconnected groups. These interactions have united the imaging community in the development of a single application for a national clinical trials network. If successful, the network will for the first time unite multiple imaging technologies and medical disciplines.
Outputs and Outcomes
In 2009, in preparation for the 2011 CIHR International review, ICR commissioned an independent impact assessment of the InstituteFootnote 11 and also of its single largest initiative, palliative and end-of-life care (PEOLC).Footnote 4 The information contained in these two documents summarizes many of ICR's achievements.
Advancing knowledge
Breakthroughs by CIHR-funded cancer researchers
Many advances have taken place in the biomedical cancer research domain, especially from researchers funded through the CIHR open competitions. Canadian researchers Dr. James Till and Ernest McCulloch were pioneers in the early discovery of stem cells. Canada continues to be a leader in this area following the elucidation of the existence and role of cancer stem cells in leukemia and brain cancer by Dr. John DickFootnote 12 and Dr. Peter DirksFootnote 13 respectively. Other breakthroughs by Canadian cancer researchers include Dr. Tony Pawson's workFootnote 14 on signal transduction in normal and cancer cells, Dr. Nahum Sonnenberg'sFootnote 15discovery of how cell homeostasis is governed through regulation of protein translation, and Dr. Tak Mak's studiesFootnote 16 lucidating tumour suppressor gene function and immunomodulation. Recent advances include decoding the genome of a metastatic breast cancer tumour by Dr. Samuel Aparicio and Dr. Marco MarraFootnote 17 and showing that it is genetically distinct from its primary tumour and Dr. David Huntsman'sFootnote 18 identification of a tumour suppressor gene that is frequently disrupted in ovarian clear-cell and endometrial tumours. Some of these discoveries have fuelled current ICR strategic initiatives towards therapeutic targets for cancer stem-like cells and new initiatives in personalized medicine.
Palliative and end-of-life care initiative
One of the measures of knowledge creation is number of publications. Canadian publications in PEOLC were steady from 2000 until the time of the PEOLC initiative, after which time the number of annual publications almost tripled, from 22 in 2003 to 63 in 2008. As the team component of the initiative funding ended only in 2009, it is highly likely that further publications are still in development.
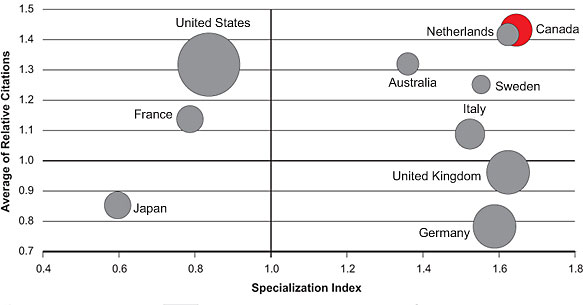
In Figure 3 the number of publications is represented by the size of the circles. A specialization index (SI) greater than 1.0 means that a particular country is more specialized in a certain area compared to the world average and an average of relative citations (ARC) of greater than 1.0 indicates that a paper or a group of papers is cited more than the world average. Publications on PEOLC were identified through Medical Subject Headings (MeSH) [searches done by the Observatoire des Sciences et des Technologies (OST)]. Databases searched may not cover all publications in this area and ARC data are incomplete for 2008. Countries were ranked based on total number of publications, 2000–2008.
Figure 3 shows that Canada scores above the world average and ranks first among the top 10 countries listed on both indices (1.64 and 1.43 for SI and ARC, respectively). Over time, ARC has increased from 1.19 at the start of PEOLC funding in 2003 to 1.72 in 2008, indicating growth over time in the citations of Canadian papers in PEOLC. These data show that for a relatively small research community, Canada's PEOLC researchers excel with respect to the quality and impact of their publications.
Figure 3: Specialization index and average of relative citations for top 10 countries publishing in PEOLC, 2000–2008
Canada now ranks first among the top 10 countries with respect to the quality and impact of PEOLC publications and level of international collaboration – a great outcome of the PEOLC initiative.
The following are examples of the new knowledge described in PEOLC publications.
Securing cost savings
Drs. Lau and Downing at the University of Victoria have developed and validated a palliative performance scale (PPS) that has provided the evidence necessary for enrolling qualifying patients into a palliative care benefits program that offers free prescriptions and other services. Further analyses have demonstrated that PPS is a strong predictor of survival in palliative patients.Footnote 19
Controlling pain
Dr. Neil Hagen's team at the University of Calgary has developed a tool to classify cancer pain that will facilitate the allocation of resources more quickly and efficiently;Footnote 20 and Dr. Pierre Gagnon's team at Laval University has developed and validated a simple instrument to assess pain in people with limited ability to communicate.Footnote 21
Access to Quality Cancer Care initiative
Although the Access to Quality Cancer Care (AQCC) initiative was funded only in late 2007, some measurable outcomes already exist.
Safer colonoscopies
An ICR-funded project focused on the complications associated with colonoscopy has generated critical information essential in the development of a population-based screening program. The project, led by Dr. Rabeneck at the University of Toronto, was the first large-scale Canadian study to focus on the risks of colonoscopy: bleeding and perforation. The project enrolled 97,091 individuals undergoing outpatient colonoscopy during a one-year period in British Columbia, Alberta, Ontario and Nova Scotia. The results indicated a bleeding and perforation rate (serious enough to require hospital admission within 30 days) of 1.64/1000 and 0.85/1000, respectively. Predisposing risk factors included older age, male sex, having a polypectomy and having the colonoscopy performed by a low-volume endoscopist. These results indicate that colonoscopy is a relatively safe procedure in Canada but that the experience of the endoscopist is an issue that will require further attention during the implementation of a national screening program.Footnote 22
Capacity building
The Institute has always been a strong supporter of the CIHR Strategic Training Initiative in Health Research (STIHR) program and ICR and partners have supported 29 cancer-related STIHRs through three competitions for a financial commitment by ICR alone of more than $20 million. In funding round three, 11 of these STIHRs were renewals of programs funded in earlier competitions. End-of-grant reports indicate that the program facilitated the recruitment of high calibre students, often from non-traditional disciplines. The trans-disciplinary nature of the training programs promoted the interaction of students with researchers from many disciplines to obtain a greater understanding of where their own research belonged in the cancer-research continuum. In some cases, such as in Nova Scotia, the capacity-building aspect of the programs has been essential to a concerted effort to create an active and vibrant cancer research community. In the words of one STIHR leader:
"Without a doubt, the ICR-funded program [STIHR grant] here was the glue that brought researchers together, acted as an incentive for recruitment of new cancer researchers, caused internal recruitment of many researchers to turn their attention to cancer issues and raised the profile of cancer research within our university and affiliated teaching hospitals. As a result, Dalhousie has been able to boast having the fastest-growing cancer research community in the country".
Capacity building in PEOLC
The PEOLC initiative focused considerable resources and national attention on a critical but previously neglected health need. The initiative built major clinical research capacity that integrated care providers and health professionals into highly applied, practice-oriented research teams.Footnote 4
The ICR PEOLC initiative transformed palliative care research in Canada by focusing considerable resources and national attention on a critical but previously neglected health need.
A small investment for a large impact
ICR launched the PEOLC Pilot Project Program ($1.3 million) so that researchers could obtain the data they needed to apply to the CIHR Operating Grants Program. It was expected that 20–25% of the pilot project grantees would succeed in future open grant competitions. A survey of subsequent grant recipients revealed that of the 18 principal investigators (PIs) of pilot project grants, 12 (66%) received an operating grant in PEOLC. In the five years preceding their pilot project award, the PIs collectively received $1.68 million in CIHR funding, while in the five years following their pilot project, they received $6.46 million – almost a four-fold increase. Of the six PIs that did not receive operating grant funding, only one had vanished; the other five were still active in the PEOLC domain and two reported having had highly productive PEOLC research careers by securing funds from sources other than CIHR.Footnote 4
Training in action
The PEOLC new emerging teams have developed a creative array of courses, seminars and Summer Institutes for their trainees. The team led by Dr. Pierre Gagnon has organized six training seminars for graduate students; three scientific days attended by more than 100 clinicians, researchers, decision makers and students; three training workshops; and 48 research conferences in Quebec City. The team also co-leads a national education initiative to implement an interdisciplinary web-based course in psychosocial oncology for Canadian graduate students.
A new generation of PEOLC researchers
As one PEOLC emerging team member said: "We started with just three of us. Now there are at least 25 team members." In the words of one of the initiative partners: "Early in the game of palliative care research, I could keep all the palliative care investigators on my speed dial. Now I don't even know how many there are – that's terrific. The next generation of investigators has been created."
Informing decision making
PEOLC's extraordinary impact
Several ICR initiatives have generated outcomes of value to decision makers. Again, the PEOLC initiative has excelled in this area. The composition of the PEOLC research community and its close ties to health care delivery have helped integrate decision makers and knowledge users into the research process. PEOLC investigators report that they have:Footnote 4
-
held focus groups with key user communities to identify issues and provide user input in protocol development and implementation
-
created community forums to share research outcomes with clinicians, family members, patients and policy makers, and suggested possible public policy and advocacy strategies
-
engaged research participants – patients and health care providers – in reviewing and interpreting the data and results
The following are specific examples of the effectiveness of the PEOLC initiative in informing decision making.
A novel form of knowledge translation
Drs. Peter Kirk and Janet Bavelas at the University of Victoria have developed a series of DVDs called Breaking Bad News that are used to train BC and New Zealand medical students as well as physicians around the world.Footnote 23 Knowledge gained from this research has been incorporated into three new palliative care guidelines to be pilot tested and ultimately sent to every general practitioner in British Columbia. This team, in partnership with another PEOLC team and the Canadian Coalition for Seniors' Mental Health,Footnote 24 has also developed delirium guidelines for palliative care patients.
Ensuring dignity in care
Dr. Harvey Chochinov and his team have developed the Dignity in Care program.Footnote 25 The Winnipeg Regional Health Authority has provided the team with an additional $0.5 million to operationalize this approach. Dignity in Care underscores the importance of core efficiencies of medical professionalism, including kindness, compassion and respect. Elements of this approach are being phased in across the Winnipeg Regional Health Authority and Cancer Care Manitoba. The research is being used to revise core regional value statements, inform organizational approaches to staff orientation; enhance staff communication skills; improve patient intake procedures that focus on aspects of personhood; utilize technology to enhance connectedness for critically ill hospitalized patients; revamp psychosocial facets of end-of-life care within personal care homes; and use web-based technologies to educate people working in health care about the challenges and opportunities embedded within Dignity in Care. The first French pilot study of dignity therapy, by another PEOLC researcher, Dr. Pierre Gagnon, showed that for the study's 26 participants satisfaction was very high (96%), with 64% reporting an increased sense of dignity.
Promoting knowledge translation – a key alliance
In 2009–2010, ICR provided funding for Knowledge Synthesis Grants in PEOLC through an open competition launched by the CIHR Knowledge Translation (KT) branch. Three of the PEOLC teams were successful in this competition, working closely with the Canadian Hospice and Palliative Care Association (CHPCA) to facilitate knowledge uptake at a national level. Throughout the PEOLC initiative, ICR has worked closely with CHPCA to facilitate a key alliance for the PEOLC community. The CHPCA is comprised of individuals, hospice and palliative care programs and services from all provinces and territories and has many dissemination and communication routes available to it. For example, the association has access to nearly 3,000 champions via e-mail, 11 provincial hospice palliative care associations, more than 530 hospice palliative care programs and services on the national directory, 11 specific listservs, and access to the Quality End of Life Care Coalition of Canada membership, including 30 national health professional and disease-specific charitable organizations. Therefore, CHPCA represents an extraordinary vehicle to ensure the dissemination and uptake of the PEOLC community's research results.Footnote 26
Health and health system/care impacts
Although changes in the health care system are slow to implement and rarely come about as a result of single studies, some of ICR's initiatives are already leading to improvements in health practice.
Improvements in palliative and end-of-life care in Canada
Online research course
A team led by Dr. Neil Hagen at the University of Calgary has developed the world's first online palliative care research methods course. Dr. Hagen reports that most palliative medicine residency programs across Canada have now made the 12-week course mandatory or strongly recommended, and the program is being adapted for medical students.
Improving treatment protocols
Dr. Shabbir Alibhai and his team at the University Health Network discovered that in patients 60 and older with acute myeloid leukemia (AML), aggressive chemotherapy was no more damaging to quality of life than less aggressive treatment approaches. The results from this project led to multi-year CIHR funding for a much larger study to investigate patient-reported outcomes in older and younger people with AML, and also to an exercise intervention study to try to improve the quality of life, fatigue and physical fitness in middle-aged and older survivors of AML treatment. The result was a province-wide study of treatment and survival in younger and older patients with AML and a consideration of aggressive chemotherapy in older AML patients.Footnote 27
Several PEOLC-funded researchers are challenging Canada's gold standard of home death, causing many organizations to reconsider their policies to better meet patient needs.Footnote 9
Access to quality cancer care – colorectal cancer screening
Educating doctors and families
Dr. Elizabeth McGregor has developed educational materials to help family physicians inform their patients about the need for colorectal cancer screening and the types of screening available. Institute funds have enabled the development of two print brochures, a website and a telephone counseling protocol to address specific barriers to screening. Dr. McGregor has since received a grant from the Alberta Cancer Board Research Initiatives Program to pilot these resources and obtain information to conduct a randomized, controlled trial that will assess the efficiency with which resources increase colorectal cancer screening uptake. Additionally, these materials will form the basis for an intervention study – funded as an ICR Emerging Team Grant in population-based colorectal cancer screening – to increase screening uptake among average-risk adults.
Economic impacts
The economic impact of improved health
Cancer is the leading cause of premature death in Canada. Based on 2009 statistics, 40% of Canadian women and 45% of men will develop cancer during their lifetimes.Footnote 28 The direct and indirect costs to the Canadian economy of diagnosis and treatment, lives lost and time lost to sickness are huge. ICR's initiatives on early diagnosis through screening, equitable access to timely cancer care and improved models of palliative care delivery can all be expected to provide outcomes that will yield economic benefits in the long term through improved cancer care. The commercialization of new products and technologies and the creation of new jobs in the research and biotechnology sectors also provide economic impacts.
Assessing the cost of PEOLC
In 2008, Dr. Pierre Gagnon's team completed a large prospective multi-site study, led by Dr. Serge Dumont, on the economic impact of end-of-life care and services.Footnote 29 A cohort of 248 patients and their main caregivers was recruited in five urban Canadian areas. These patients were followed from entry into the program to their death or up to a maximum of six months. The study provided comprehensive knowledge of costs incurred by palliative care patients and their families. It also evaluated how these costs were shared between government, families and non-for-profit organizations. A second phase is planned to address this issue in rural areas of three Canadian provinces. The recruitment of participants began in February 2009. These two studies will shed light on the economic consequences on family and close friends of caring for a dying loved one and will provide the evidence necessary to re-evaluate models of care delivery in PEOLC.
Cost savings through prevention and early diagnosis
One of the projects funded as part of ICR's colorectal cancer initiative, led by Dr. Linda Rabeneck, brought together a team of researchers, educators and health policy makers from Ontario, Alberta, the United States and the Netherlands to provide evidence on how best to implement currently available screening tests in Canada at a population level. This international team has completed the first population-based Canadian estimates of the attributable costs of colorectal cancer, which will be used to develop a screening cost-effectiveness model. This work was presented in June 2010 at the Bienniel International Cancer Screening Network meeting in Oxford.Footnote 30
Attracting additional funds
Dr. François Bénard's team, funded under ICR's first imaging initiative, the Novel Technology Applications in Health Research, reports that the funds helped foster multidisciplinary collaboration between physicians, PET and MRI physicists, radiochemists and cancer biologists to develop new multimodality approaches to cancer imaging. The group went on to receive further long-term support through a CIHR resource grant that has resulted in three patent applications and the start-up of two commercial activities. Another team in this initiative obtained a larger New Emerging Team Grant on quantum dot-based biomolecular imaging and this biophotonics group is now part of a Canadian Foundation for Innovation grant and a CIHR Team Grant.
"The Novel Technology Applications in Health Research RFA was the prime stimulus for creating the team effort. It also accelerated the expanding nanomedicine program in Toronto leading to new diagnostic and therapeutic approaches in cancer and other diseases that ultimately will help the emerging Canadian nanotechnology industry sector."
Transformative effects of the Institute
The ICR niche
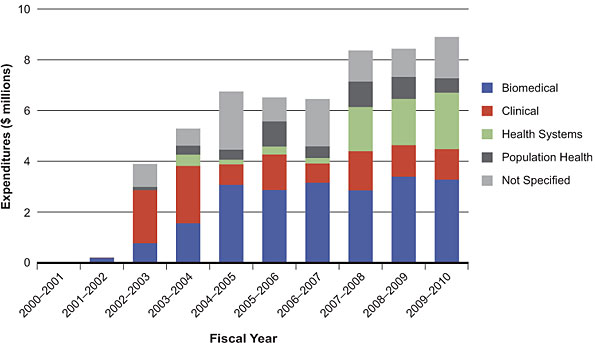
For 2009–2010, approximately 86% of CIHR cancer-related funding in the open competitions supported biomedical research. The distribution of ICR strategic research funding across health themes (Figure 4) differs dramatically from the overall CIHR distribution with only 37% supporting biomedical research in 2009–2010 and 45% supporting clinical, health services and population health research (18% with research theme unspecified). This reflects ICR's early recognition of the need to be strategic and invest where the greatest impact might be felt. The sudden increase in clinical research funding in 2002–2003 and 2003–2004 represents ICR's partnership with the National Cancer Institute of Canada to support cancer clinical trials, and the continuing investment in clinical research is due primarily to the Institute's PEOLC initiative. The jump in funding for health systems research in 2007–2008 is due to the funding of the Access to Quality Cancer Care initiative.
Figure 4 is based on the discipline identified by the principal applicant at the time of application. The Not Specified portion reflects those applicants that did not indicate a primary research field.
Figure 4: ICR investment in cancer research by theme, 2000–2010
ICR found its niche by focusing on underserved areas of health research in the clinical and health services domains, transforming the cancer research landscape in these areas.
To date, the most transformative of ICR's initiatives has been the PEOLC initiative. This initiative focused significant resources and attention on a previously neglected area of health research and, through a suite of specialized program tools, built clinical research capacity that increased both the quantity and quality of PEOLC research many-fold.Footnote 4 The teams formed through this initiative are excellent examples of integrated knowledge translation in action as most have developed strong and effective partnerships with user communities, including decision makers and patients. In many cases, team members were already experienced health practitioners or decision makers and so were able to implement change directly. The initiative has attracted many communities and collaborators from outside mainstream academia who would not have been eligible for CIHR funding, but who have made major contributions to the field. The initiative has also had a dramatic impact on the degree of collaboration between Canadian PEOLC researchers. This is well illustrated in Figure 5 below, which illustrates the effect of the ICR PEOLC initiative on collaborations and number of co-publications among PEOLC researchers.Footnote 4
Figure 5: Co-publications among members of PEOLC New Emerging TeamsFootnote 4
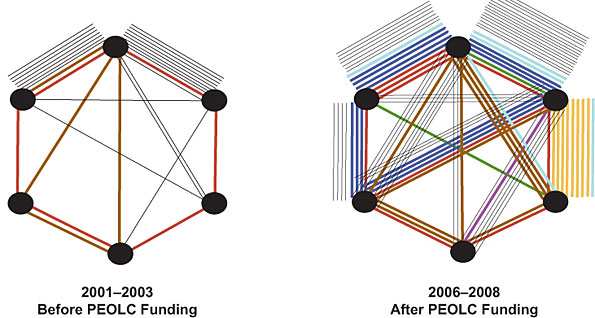
Each team is represented by a different colour. Each black dot represents one principal investigator (PI) of a team up to a maximum of six per team (some teams had less than six PIs). Each line represents a co-publication between team members. The thin black lines represent non-palliative care co-publications, while coloured thick lines represent palliative care co-publications. Data are from the Scopus database using the search terms: "palliative care" affiliation: "Canada".
From 2001 to 2003, before PEOLC funding, the members of only two teams (red and brown) had co-published papers in palliative care. Between 2006 and 2008, the number of co-publications among team members had increased dramatically, a trend that will continue as more publications appear.
ICR's role in changing the Canadian cancer-research landscape
Despite its modest budget and small staff, ICR has had a considerable impact on the Canadian cancer research landscape, primarily through the extraordinary abilities of its founding scientific director, Dr. Philip Branton. ICR, under Dr. Branton's leadership, established the first cancer research alliance in 2003, which became the Canadian Cancer Research Alliance (CCRA). Under ICR's direction, CCRA developed the first report to record annual cancer research investment in Canada. This yearly report provides a snapshot of cancer research funding by organization and province as well as by tumour site and discipline, and serves as a valuable resource for the cancer community.Footnote 1 The ICR goal was to create a national vision for cancer research that could support large-scale, multidisciplinary, national initiatives beyond the scope of individual organizations acting independently. The two initiatives originally identified eventually received funding through the Canadian Partnership Against Cancer Corporation (CPACC)–The Canadian Partnership for Tomorrow Project, a long-term population-based cohort and a translational research initiative funded by CPACC in partnership with the Terry Fox Research Institute. CCRA has now become the CPACC Research Advisory Group, and is financially supported by CPACC. CCRA is still co-chaired by ICR's scientific director.
ICR has exerted a considerable influence on the direction of Canadian cancer research through the creation of alliances between stakeholders.
Going Forward
Building on lessons learned
Over 10 years, ICR has learned the value of carefully targeting areas of research in which the Institute can have a significant impact. ICR has also learned the value of collaborating with the broader cancer-control research community to align priorities, reduce duplication and leverage strategic funds. The Institute's most successful initiatives have been based on these principles and have benefited from engaging the end users of research from the beginning of the research process. ICR will continue to work closely with members of the Canadian Cancer Research Alliance (CCRA) and align Institute initiatives with the CCRA national strategy and CIHR's strategic plan. The unifying theme for ICR activities will be research excellence and innovation, and the Institute will continuously monitor new developments in cancer research for opportunities to assist the broader community in achieving the best possible research outcomes.
Supporting early initiatives
The Institute will monitor the outcomes of all its initiatives to inform future directions. The Palliative and end-of-life care (PEOLC) initiative built capacity, creating a new generation of alliances and partnerships. It is hoped that the PEOLC peer review committee will facilitate continued funding for this group through CIHR open competitions. ICR has committed funds to sustain the unique research networks created by PEOLC in a new program developed by the CIHR Knowledge Translation Branch and launched in August 2010.
Addressing new priorities
As part of the 2010–2015 ICR strategic plan, the Institute will work closely with other CIHR Institutes and external partners to create large, multi-theme, multidisciplinary initiatives likely to have an impact on the health of Canadians. Cancer research falls primarily within the CIHR priority area 1, Enhance patient-oriented care and improve clinical results through scientific and technological innovations, and priority area 5, Promote health and reduce the burden of chronic disease and mental illness. ICR initiatives will also address other CIHR priority areas. In future, ICR will focus on the research areas described below.
Cancer prevention – Lifestyle, environment and cancer
Many potentially modifiable causes and risk factors for cancer have been identified. These include lifestyle factors such as diet, inactivity, obesity and the use of tobacco products, and environmental factors such as exposure to carcinogens and cancer-causing microbes.Footnote 31 There is increasing evidence that many such factors promote chronic inflammation and that inflammatory responses are associated with the etiology of many chronic diseases, including cancer.Footnote 32 ICR's approach to prevention research will centre on partnerships with other CIHR institutes and external partners. Together, ICR and partners will develop studies for understanding the impact of chronic inflammation in cancer initiation as well as epidemiological and intervention studies, some of which will take advantage of the large and well annotated population-based cohort studies and bio-repositories that now exist in Canada.
Diagnosis and guided therapy: towards personalized medicine
The application of genomic knowledge has dramatically increased our understanding of cancer biology. It is now evident that cancers are heterogeneous cell populations that include multiple tumour subtypes in addition to stromal and inflammatory cells and their products. Patients with apparently similar cancers may respond quite differently to the same treatment. Increasingly, new therapies are targeted at those patients whose tumours are predicted to respond; such therapies are effective in only a subset of patients. This creates the challenge of how to tailor treatments for the specific patient sub-populations that will be responsive. ICR is leading the development of a multi-institute initiative that will focus on the application of new technologies, biomarkers and strategies to improve patient stratification and treatment, and on the complex ethical, economic and health service and system challenges integral to the personalized medicine approach. One aspect of interest to ICR is the possibility of using the new generation of imaging technologies to validate biomarkers of disease and evaluate therapeutic response.
Targeting cancer-initiating cells
Recent evidence suggests that many cancers contain a small sub-population of tumour-initiating or cancer stem cells. These are highly resistant to the standard cancer treatments of chemotherapy and radiation and are responsible for maintaining the bulk tumour and establishing metastatic disease. In October 2009, the Cancer Stem Cell Consortium (CSCC) funded two large Canada–California research teams, led by Drs. John Dick and Tak Mak, for an investment of $40 million over four years. The teams will develop cancer stem-cell targeted therapies to be ready for clinical trials within four years. In collaboration with other CSCC members, ICR now plans to develop initiatives to further explore the basic characteristics of cancer stem cells and the storage and retrieval of live cancer stem cells. This initiative will promote development of new reagents, tools and technologies aimed at molecular understanding and therapeutic interventions and provide the necessary platforms and infrastructure to advance and sustain Canadian cancer stem cell research.
Cancer survivorship
Although improved cancer management has increased the number of cancer survivors, many of these survivors live with debilitating side effects caused by aggressive cancer treatments. This is particularly true in the pediatric, adolescent and young adult population who, because of their age at diagnosis and the success of current treatments, can be expected to live for many years. Although more than 80% of pediatric and adolescent cancer patients survive their disease, many suffer severe, sometimes fatal side effects that can manifest decades after the primary treatment. One challenge is to establish a dialogue between the pediatric oncologists and the specialists treating the late effects, often years later. Building on previous experience in uniting research communities, ICR launched in June 2010 an initiative to address this issue called Childhood Cancer: late effects of treatment. Another challenge is relating individual genome signatures to treatment responses and risk of adverse effects. To address this challenge, ICR is collaborating with Genome Canada and the CIHR Institute of Genetics in an initiative that will provide the pediatric research community with access to third-generation genome sequencing platforms. These studies will advance our understanding of the genetic profiles of pediatric diseases, including cancers and the correlates of treatment response.
ICR guiding principles
Building on lessons learned, and taking into account recommendations forthcoming from the 2011 CIHR International Review, ICR will focus on innovative, strategic approaches and programs that will build on the cadre of outstanding cancer researchers funded in the open competitions and the wealth of infrastructure and research platforms that exist across the country. By serving as a catalyst, ICR can facilitate research that would be difficult or impossible to support otherwise. ICR will adapt the strategies and principles that guided previous initiatives to provide a stronger focus on integrated knowledge translation and increase the impact of new initiatives. ICR will incorporate ethical considerations, especially in the domain of personalized medicine where the ethical issues are highly complex.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
ICR specific
| AML | acute myeloid leukemia |
| AQCC | Access to Quality Cancer Care |
| ARC | average of relative citations |
| CAPCA | Canadian Association of Provincial Cancer Agencies |
| CCRA | Canadian Cancer Research Alliance |
| CHPCA | Canadian Hospice and Palliative Care Association |
| CPACC | Canadian Partnership Against Cancer Corporation |
| CSCC | Cancer Stem Cell Consortium |
| CTRNet | Canadian Tumour Repository Network |
| IAB | Institute Advisory Board |
| KT | knowledge translation |
| MeSH | U.S. National Library of Medicine Medical Subject Headings |
| NCIC | National Cancer Institute of Canada |
| NCRI | National Cancer Research Institute |
| NSERC | Natural Sciences and Engineering Research Council |
| OST | Observatoire des Sciences et des Technologies |
| PEOLC | palliative and end-of life care |
| PI | principal investigator |
| PPS | palliative performance scale |
| RFA | request for applications |
| SI | specialization index |
| STIHR | Strategic Training Initiative in Health Research |
- Date modified: