ICRH Strategic Plan 2013-2016
September 8, 2014
Final version
Table of Contents
- 1. Executive Summary
- 2. Mission, Mandate, and Values
- 3. The Present Context
- 4. ICRH Objectives and Strategic Priorities for 2013–2016
- 4.1 ICRH Objectives
- 4.2. Strategic Priorities for 2013–2016
- 4.2.1 Priority 1: Enhance Capacity, Competitiveness, and Impact through Networking
- 4.2.2 Priority 2: Training Mentoring, and Early Career Development to Promote Capacity Building
- 4.2.3 Priority 3: Enhance Opportunities for Clinical, Population Health, and Health System/Services Research through Cohort Linkage and Data Enhancement
- 4.2.4 Priority 4: Contribute to the Advancement of Relevant CIHR Roadmap Signature Initiatives
- 5. Conclusions
- References
- List of Figures
- Figure 1: CIHR Strategic Priorities and Roadmap Signature Initiatives
- Figure 2: Cost/burden of disease
- Figure 3: Relative growth in number of funded grants/awards from 2000/01 to 2012/2013 according to Institute
- Figure 4: Total funds awarded through OOGP grants per ICRH mandated field
- Figure 5: Evolution in number of funded trainees per ICRH mandated field
- Figure 6: Proportion of funding according to four CIHR themes
- Figure 7: Relative change in number of cardiovascular clinical trials publications since 1997 on an annual basis, comparing the top 10 countries
1. Executive Summary
The Institute of Circulatory and Respiratory Health (ICRH) - one of the 13 Institutes of the Canadian Institutes of Health Research (CIHR) – supports research that focuses both on the health of major organ systems and related diseases, and on a variety of chronic diseases with the largest societal and economic burden. This reality, and the extraordinary diversity of these medical conditions, presents a major operational challenge for ICRH. Despite these difficulties and limited resources, the Institute’s 2013-2016 Strategic Plan demonstrates a commitment to ensuring that research excellence, capacity, competitiveness, innovation, and impact are enhanced across all research fields affiliated with the Institute, including: cardiovascular health, respiratory health, blood, blood vessels, stroke, critical/intensive care, and sleep/circadian rhythms. Moreover, building on previous successes, ICRH will continue nurturing past collaborations and work to establish new meaningful national and international alliances with the research community, partners, and other stakeholders to develop interdisciplinary, integrative health research that reflects Canada’s emerging health needs, gaps and opportunities. ICRH will also strongly support partnerships with relevant stakeholders to accelerate the transfer of new knowledge into benefits for Canadians. Notably, patient engagement will be an important priority that will serve as one of the major building blocks of all ICRH clinically related initiatives.
Based on identified gaps, opportunities, and feedback received from the International External Review Panel (CIHR’s 10-year International Review), ICRH research communities and partners, and in alignment with CIHR’s 2014-2018 Strategic Plan (Health Research Roadmap II), ICRH has identified four research priorities for the upcoming years. The first priority will focus on enhancing capacity, competitiveness, and impact of our communities through networking. This objective is consistent with the importance of aligning with CIHR’s largest comprehensive Signature Initiative - the Strategy for Patient-Oriented Research (SPOR). Emerging Networks will be developed in three pre-identified gap areas: respiratory health, vascular health, and stroke prevention through Atrial-Fibrillation (AF) clinical trials. In addition, ICRH will target four specific areas for the establishment of Focused Community Development Programs in critical care, stroke treatment and recovery, sleep and circadian rhythms, and blood diseases. In alignment with CIHR’s Citizen and Patient Engagement Framework, through these programs, ICRH will pursue specific actions to enhance patient-engagement in health research and implement patient-engagement as a core priority in strategic initiatives by developing a set of programs and tools that will allow patients to be true partners in research. Finally, ICRH will continue its collaboration with the National Heart, Lung, and Blood Institute (NHLBI) of the National Institute of Health (NIH) in the ongoing support of two large Canada-US networks – the Resuscitation Outcomes Consortium (ROC) and the Cardiothoracic Surgical Network (CTSN), and will explore other opportunities for networking at the international level.
ICRH’s second priority will target training, mentoring and early career development to promote capacity building – areas of need that CIHR has also recognized as requiring specific attention. For ICRH, recent data has demonstrated that since the inception of CIHR, the growth of funding within Institute mandated research areas has been slower than in all other areas at CIHR, in particular for the cardiovascular and respiratory communities. Evidence suggests this is primarily due to declining numbers of young investigators. The development of research capacity related to health systems/services and population/public health, as relevant to ICRH research areas, has been identified as requiring particular attention.
In the upcoming years, ICRH will work closely with relevant CIHR Institutes and working groups to address this important and persistent capacity problem, focusing both on training/mentoring issues, as well as on issues impacting early career success of young investigators. ICRH will also continue working with partners and various stakeholders to develop a joint, comprehensive strategy that will directly align with at least some elements of partner-led programs.
ICRH’s third priority will focus on the expansion of opportunities for clinical research, health systems/services research, and population health through cohort linkage and data enhancement. Such an initiative will provide Canadian scientists with a unique opportunity to boost knowledge development and translation at a fraction of the cost of developing new cohorts. The linkage and enhancement of, existing cohort data will enable Canada to better develop population-based research and design individualized and community-based prevention and/or intervention programs. In addition, cohort linkage and data enhancement will contribute to improving the potential for health and health systems research by creating a formidable pool of population-based data that can be linked to Canada’s uniquely powerful administrative databases. Data enhancement and linkage will also directly assist in gathering and analyzing important, yet sparse, data related to Canada’s Aboriginal Peoples and other vulnerable populations. Finally, by helping to address issues such as data storage and access policies, this initiative will support research on ethics. Along with CIHR and its other Institutes, ICRH will help coordinate disparate and multidisciplinary communities to bridge gaps and identify ways for harmonizing, and sharing population-relevant data sets and their efficient utilization. In the context of increasing prevalence of many cardiovascular and respiratory risk factors, many of which are also risk factors for serious and chronic diseases in other fields, this initiative provides a unique opportunity for the ICRH community to link with other CIHR communities in building tools to fuel clinical research as well as, population health, health services, and policy research.
The Institute identified contribution to the advancement of relevant CIHR Roadmap Signature Initiatives (RSI) as its fourth priority. ICRH anticipates these large-scale, multi-Institute programs will bring the Canadian scientific community together and will transform research in selected areas on a national and international scale. Importantly, a number of these comprehensive programs, such as the SPOR RSI, directly align with ICRH priorities; thus, ICRH will work closely with CIHR and its Institutes to advance these major initiatives. For example, to support the Inflammation in Chronic Disease RSI, ICRH is funding research on inflammation and respiratory diseases through the Health Challenges in Chronic Disease program. Moreover, ICRH supports the development of the Canadian National Transplant Research Program in partnership with the CIHR-Institute of Infection and Immunity and multiple other partners. In support of the Personalized Medicine RSI, ICRH will contribute to specific projects (i.e. those aligned with any of the ICRH Emerging Networks) – that are funded through the Genomics and Personalized Health program. In relation to the International Collaborative Research Strategy for Alzheimer’s Disease RSI, ICRH will contribute funding towards the development of an integrated consortium-based research program that will incorporate the appropriate vascular elements and their role in the development of cognitive impairment. ICRH through its cohort linkage and data enhancement priority will support the Pathways to Health Equity for Aboriginal Peoples RSI.
In close collaboration with CIHR’s Institute of Aboriginal People’s Health and the Heart and Stroke Foundation, ICRH will contribute to the development of a cohort that will aim at thoroughly phenotyping a sample of Aboriginal individuals living on reserves. This undertaking will create an important resource for researchers and will be useful for developing and assessing programs designed to improve the health and health care of these communities. Finally, through the emerging Environments & Health RSI, ICRH will create opportunities to link a wide array of potential environmental health determinants to large, well-characterized cohorts, that in turn are to be linked to health care utilization and outcomes, and enriched with phenotypic, biomarker and other information useful for assessing individual as well as population-level risk. This initiative will increase the use of existing cohorts, improve sustainability of such cohorts, and create a national resource for conducting environmental health research in Canada.
The Institute of Circulatory and Respiratory Health is in a strong position to guide the shaping of the Canadian research landscape over the next few years. By working closely with its research communities and partners on common pressing issues such as increasing research capacity through networking, training/mentoring/career development, cohort linkage and data enhancement, ICRH will continue to demonstrate its leadership and commitment to knowledge development and translation and will be supporting research excellence aimed at reducing the burden of disease in Canada. Importantly, ICRH will work closely with CIHR to support and foster active engagement of patients at all levels of research within its communities to lead the way in transformative patient-oriented research.
2. Mission, Mandate, and Values
The Institute of Circulatory and Respiratory Health (ICRH) is one of the 13 Institutes of the Canadian Institutes of Health Research (CIHR), and as such must support CIHR’s mission, mandate and strategic plan when establishing its future plans and programs.
2.1 The Mission of CIHR
The mission of CIHR as expressed in the CIHR Act that created it, is to “excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system”.1
2.2 The Mandate of CIHR’s Institutes
The mandate of CIHR’s Institutes as outlined in the CIHR Act is “together pertain to all aspects of health, include biomedical research, clinical research, research respecting health systems, health services, and the health of populations, societal and cultural dimensions of health and environmental influences on health and other research as required, work in collaboration with the provinces to advance health research and to promote the dissemination and application of new research knowledge to improve health and health services, and, engage voluntary organizations, the private sector and others, in or outside Canada, with complementary research interests”.
2.3 The Mission of ICRH
The mission of ICRH is to support CIHR’s mission by “supporting research into the causes, mechanisms, prevention, screening, diagnosis, treatment, support systems and palliation for a wide range of conditions associated with the heart, lung, brain (stroke), blood vessels, blood, critical and intensive care, and sleep”.2
2.4 The Mandate of ICRH
The mandate of ICRH is to ensure that research excellence, capacity, competitiveness, innovation, and impact are maintained across all research fields affiliated with the Institute, including: cardiovascular health, respiratory health, blood, blood vessels, stroke, critical/intensive care, and sleep/circadian rhythms as outlined in CIHR’s act.
2.5 Values that Guide ICRH
- Excellence
- Rigor
- Respect
- Responsibility (including social responsibility)
- Innovation
3. The Present Context
3.1 Global Perspective
Despite the economic downturn of the last few years, investment in health research in most western countries has generally been maintained, and in some cases has even increased. Nevertheless, because of continued economic uncertainty and the need for countries to reduce their deficits and debt despite a stagnant economy, it is unlikely that significant increases in funding are forthcoming, and there is a real risk of reduced funding in the near future.3 This situation exerts added pressure on research funding organizations that are tasked both with supporting research that addresses key knowledge gaps, evaluates return on investment in improving health, creates wealth, and reduces the costs of health care in the country they serve. Indeed, the persistently greater rise in health costs than would be expected with inflation and change in GDP has progressed to a level that is unsustainable, which puts the fragile economy of many countries at further risk.3
International collaboration: As with other sectors, health-related research has become progressively more global, involving a growing number of collaborative efforts among scientists from different regions and countries. This is also true in Canada.4 Such partnerships, whether international or more national in scope, encourage collective identification of the most pressing knowledge gaps in a given field; integration of multi-disciplinary expertise; optimization of the use of essential, sophisticated, and costly equipment; increase the impact of health research by partnering with regional organizations that can facilitate knowledge translation and technology transfer; and increase the value for money in health research. Despite much progress in the development of international research, achieving research excellence is impeded by the complexity of structuring and co-funding of large national and international studies.5
Innovation and Knowledge Transfer: Presently, there is widespread realization a growing gap exists between discovery and our ability to bring these discoveries to the service of populations, patients and the health care system.6–7 Despite the dramatic increase in scientific publications in health research, there is a dearth of new therapeutic agents and targets - a situation threatening the ability of the biopharmaceutical industry to develop and market new therapies that offer significant improvement over existing ones. This situation leads to questions about the effectiveness of present innovation processes and the presence of adequate links between (academic) research and industry.
Patient-Oriented Research: Over the past several years, growing concern has been expressed regarding the responsibility of bringing evidence-based best practices to individual patients at the right time, and the need to optimally organize health care to better meet the needs of patients and of society. This realization has led many countries to develop strategies to reinforce knowledge translation and better support patient-oriented research targeting these problems. For example, the funding of patient-oriented research in the UK exceeded $1.6 billion in 20118 and continues to grow.
A critical step to conducting research that is truly patient-oriented is the engagement of patients as partners within the research enterprise. This begins with recognizing the patient’s experience-based knowledge in the research process and extends beyond to involve patients at all levels of research including research development, planning, decision-making, operations and knowledge translation.
Increasingly research teams involve patients at the early stages of their working process to improve the relevancy of the research, stay focused on population needs, enhance research design, multiply ways of accurately capturing experience-based knowledge, and to facilitate knowledge transfer and participative research. Unfortunately, the gap between patient engagement in research and perceived best practices in this field remains great in many areas.
Bridging this gap requires a culture shift that moves beyond the role of patient-engagement in research as advocates for improved care (although advocacy remains important), to a view of patients as knowledge experts and dynamic actors within the research process. In this view, patients can be co-researchers, coaches, trainers and even co-leaders of research.
In alignment with CIHR’s Citizen and Patient Engagement Framework, ICRH will pursue specific actions to enhance patient-engagement in health research and implement patient-engagement as a core priority in our strategic initiatives. We will work with CIHR, researchers, and patients to develop a set of programs and tools that will allow patients to be true partners in research. This will be done in the following ways:
- ICRH Networks & Community Development programs will be required to engage patients in a formal way, including:
- Plans for patient engagement in their governance models;
- Patient(s) on the Executive Committee of the Network and on the Steering Committees of each of the clinical trials undertaken by the Program;
- The training of patients in optimal patient engagement in research;
- The training of researchers in optimal patient engagement in research;
- Active engagement of patient representatives in research planning and decision making;
- Patient-engagement plans and patient-oriented knowledge transfer activities that will ultimately change patient outcomes; and
- Formal evaluation of patient needs in the designing of research projects.
- A series of community webinars developed by ICRH, CIHR and experts in patient-engagement to educate research leaders on the added-value of engaging patients throughout the research process, and to provide best practices tools to researchers on how to consult, involve and partner with patients, and on how to train patients to be effective research partners.
- Emphasis on patients as co-builders of research and research projects.
By integrating patients as partners in the development of research strategies and programs, ICRH’s research communities will lead the way in transformative patient-oriented research and benefit from patient involvement to improve the relevance and impact of research on health and well-being, clinical practice, and to contribute to more effective health services, policies and products.
3.2 Canadian/CIHR Perspective
The global research environment has invariably influenced the Canadian research environment. Despite a substantial increase in health research funding in Canada since 2000 (CIHR’s total budget has progressed from $280 million in 1999 to more than $860 million in 2006), Canadian health research funding has levelled off and, when inflation is factored in, health research funding in Canada has actually diminished over the last five years. As both the Canadian Federal and Provincial governments struggle to balance their budgets in the face of stagnant economies and existing deficits, it is unlikely that funding for health-related research will grow rapidly over the next few years. In some jurisdictions, the annual rate of health research funding may even further decrease. Understandably, greater accountability and a more strategic use of existing funds are expected, as well as better leveraging of existing funds through partnerships. Despite these challenges, CIHR has wisely committed to protecting and, even increasing the funding for the Open Operating Grants Program (OOGP) - the cornerstone of research at CIHR.
Consistent with the need to strategically focus its resources, CIHR has chosen to focus on 3 Strategic Directions, as outlined in the 2014-2018 CIHR’s Strategic Plan or Health Research Roadmap II:
-
Strategic Direction 1: Promote Excellence, Creativity, and Breadth in Health Research
- Goal 1: Support leading researchers and important advances in health
- Goal 2: Build a solid foundation for the future
-
Strategic Direction 2: Mobilize Health Research for Transformation and Impact
- Goal 1: Refresh health and health systems research priorities
- Goal 2: Reap benefits through strategic alliances
-
Strategic Direction 3: Achieve Organizational Excellence
- Goal 1: Enhance transparency and accountability
- Goal 2: Ensure responsible governance and stewardship
- Goal 3: Build a modern, world-class work environment
* These CIHR Strategic Directions will be referred to throughout the document as *CIHR Strategic Direction 1, 2, and 3.
To achieve international excellence, and consistent with the need to network and focus resources, CIHR’s Roadmap II identified four major research priority areas which will:
- Enhance patient experiences and outcomes through health innovation;
- Health and wellness for Aboriginal peoples;
- Promote a healthier future through preventive action; and
- Support research to improve quality of life for persons living with chronic conditions.
To address these research priorities and achieve greatest impact while maximizing its strategic investment, CIHR launched a process to identify and develop large scale, multi-Institute programs, the Roadmap Signature Initiatives (Figure 1). Following environmental scans and extensive consultations, eight Signature Initiatives were approved and are now in the process of being rolled out. It is expected that this slate of programs – which will be primarily funded by the 13 Institutes and their external partners - will bring the Canadian scientific community together and transform research in these areas on a national and international scale.
Figure 1: CIHR Strategic Priorities and Roadmap Signature Initiatives
| CIHR Priorities | Roadmap Signature Initiatives |
|---|---|
Footnotes
|
|
| Enhance Patient experiences and outcomes through health innovation |
|
| Support Health Equity and Wellness for Aboriginal Peoples |
|
| Promote a Healthier Future through Preventive Action |
|
| Support Research to Improve Quality of Life for Persons Living with Chronic Conditions |
|
3.3 ICRH Perspective
3.3.1 Burden of Disease
ICRH has within its mandate the largest cost burden of diseases (Figure 2), as compared to the other 12 Institutes at CIHR. In addition, the Institute supports research that focuses on the health of major organ systems and related diseases, including: atherosclerosis, heart failure, stroke, asthma, sleep apnea and chronic obstructive lung diseases. This reality and the extraordinary diversity of such medical conditions present a daunting organizational and strategic research challenge for ICRH.
Figure 2: Cost/burden of disease9
Cost due to disease10 for the leading 20 diagnostic categories, by direct11, and indirect costs12, Canada, 2000
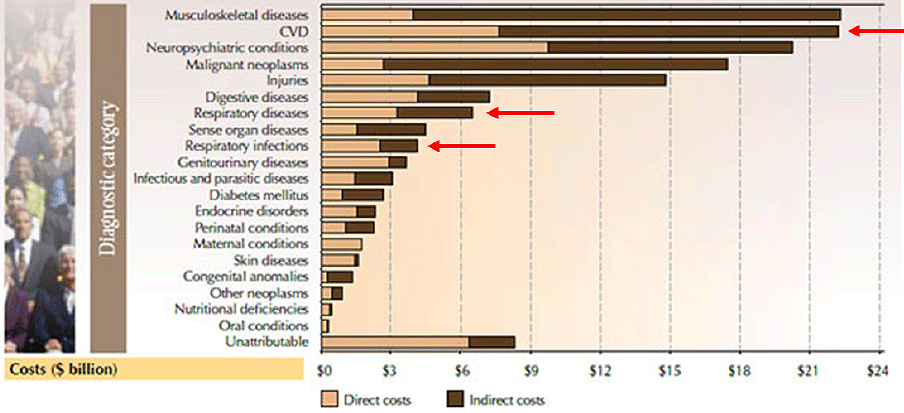
Although advances in the therapy of cardiovascular diseases have accounted for an overwhelming majority of the increased longevity of people in Canada and the US over the last 30 years13, it is anticipated that cardiac ischemic disease will become the leading cause of death and disability world-wide by 2020 because of the rapidly increasing prevalence of risk factors for cardiovascular diseases globally. Other diseases included under ICRH’s mandate are also major sources of morbidity and mortality, with cerebrovascular disease being the fourth most common cause of death and disability (and a known factor in the development of cognitive impairment), chronic obstructive pulmonary disease as the fifth, and lower respiratory tract infection as the sixth most common cause of death and disability worldwide. Importantly, the development of many chronic respiratory diseases is still not well understood, posing a real challenge to our ability to impact health outcomes. By 2020, it is anticipated that 5 out of the 7 most important causes of death and disability worldwide will fall within the ICRH’s mandate.14
3.3.2 Recommendations from the 2011 International External Review Panel (ERP)
As with the other CIHR Institutes, ICRH’s progress from 2005-2010 was assessed by an External Review Panel (ERP) as part of CIHR’s International Review. The ERP provided an assessment of the progress of ICRH, and recommendations to guide its future development.15 Overall, the ERP was favorably impressed by the influence that ICRH has had on both the quantity and quality of health-related research within its mandate. On the basis of available data, they concluded that, since ICRH’s inception 10 years ago, and, particularly more recently, research activity has adopted a greater translational direction towards public and patient benefit. This was achieved by the catalytic influence of the Institute in encouraging multidisciplinary, multi-institutional and multi-partner funded research that was especially effective in circulatory diseases, but less so in lung diseases, blood and sleep. However, in each of these latter fields the ERP perceived new activity in the right direction. It was the panel’s view that by establishing a firm productive translational agenda with support for clinical and health systems scientists, ICRH had provided the substrate for increasing Canada’s international competitiveness in health research and its beneficial impact on patients. These successes notwithstanding, the ERP had several important recommendations:
- Networks: The ERP remarked that the development of Networks in areas under the ICRH mandate catalyzes the development of the ICRH community and would be an excellent tool to impact the greatest number of researchers who are part of ICRH’s broad mandate. They added “we wish to strongly encourage further activities of this type not only in cardiovascular disease but in lung, blood and sleep”.
- Capacity Building: The ERP expressed concerns regarding the training and career development of young researchers. They understood that this was a challenge that required the collaboration of many stakeholders, of which ICRH was a reasonably small yet important player. The ERP went on to stress that “the right balance of research expertise to populate and drive forward these large initiatives is essential as is ensuring a strong pipeline of young, diverse and skilled researchers”.
- Clinical Trials: The ERP commended the great productivity of cardiovascular researchers in performing meaningful clinical trials. However, they commented: “we would encourage a wider spread of trials across the Institute’s disease areas and greater international engagement with countries beyond the US.”
- Governance: The ERP alluded to the need for greater transparency and inclusiveness in setting the research priorities of the institute, stating: “greater openness and inclusiveness in research priority setting should also help deliver high quality outcomes in these disease areas where there remains considerable unmet clinical needs set against an aging population, changing lifestyles and living with environmental change.”
3.3.3 Additional challenges and opportunities for ICRH
(i) Comparatively slow growth in grants and awards competitions
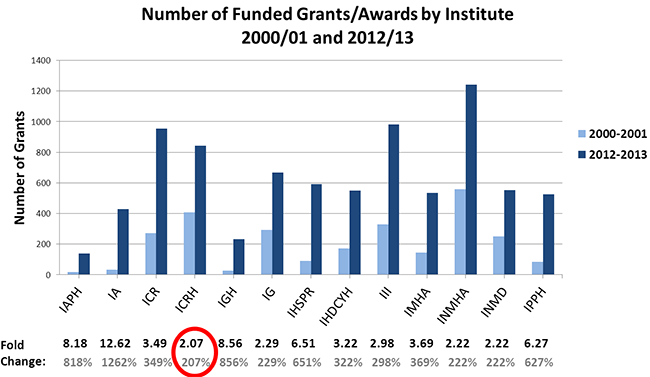
Data extracted from the CIHR database clearly indicates that during the 2000-2013 period, the relative growth in total grants and awards (CIHR Open Competitions) identified as relevant to ICRH’s mandate, was the smallest among all other CIHR institutes. In fact, while the growth fold change in total grants and awards from 2000 to 2013 for ICRH was 2.07, the fold change of other institutes ranged from 2.22 to 12.62 (Figure 3). This increase is also the smallest in relation to other disease-based domains of research (i.e. cancer, infection-immunity, and neurosciences/mental health/addiction). This is particularly alarming, given the heavy and increasing burden of disease that is covered under the ICRH mandate.
Figure 3: Relative growth in number of funded grants/awards from 2000/01 to 2012/13 according to Institute
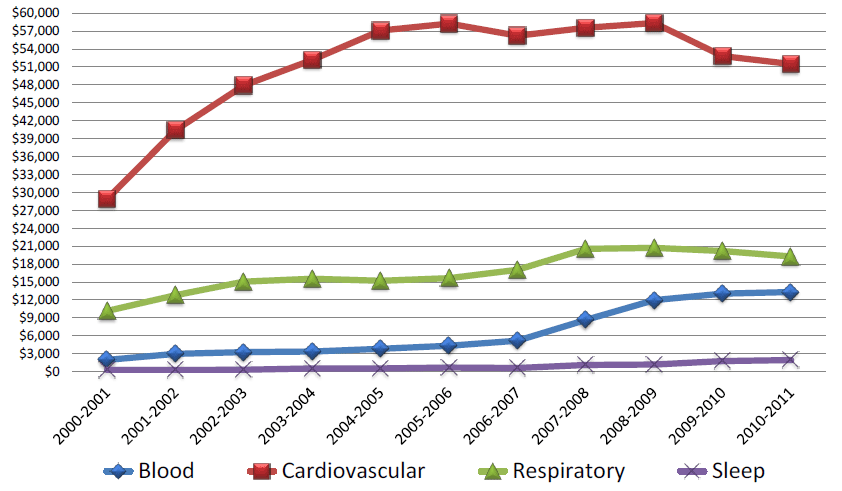
This relative lack of growth varies markedly according to the community served within ICRH. Since 2004-2005, the total funds awarded through OOGP grants in cardiovascular health has remained stable or decreased, while a similar trend in respiratory health is evident beginning since 2007-2008. The smaller communities of blood and sleep have experienced moderate increases in total funds awarded through the OOGP (Figure 4). As will be described below, this situation seems to be related to a relative lack of growth in capacity (fewer young investigators) and to a lesser extent, to issues of balance across pillars and competitiveness in certain strategic research competitions.
Figure 4: Total funds awarded through OOGP grants per ICRH mandated field
(ii) Shortage of trainees and young investigators
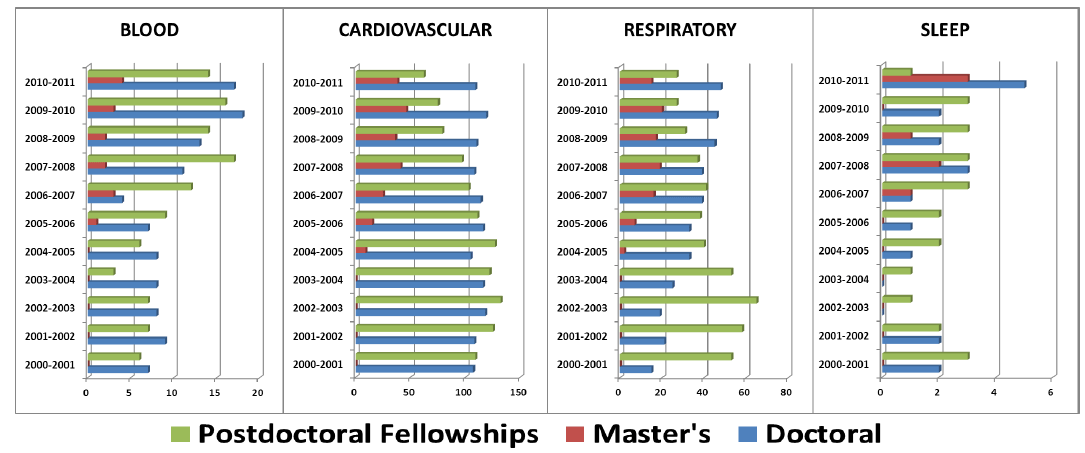
According to CIHR data compiled for the period of 2000 to 2010, the number of training award applications from the ICRH community has increased by a mere 30%. while the number of applications to CIHR overall increased by 75% during the same period. Notably, the success rates for candidates from the ICRH community and other CIHR communities were generally comparable. Thus, the problem appears to relate to the relatively low number of applicants, with the number of ICRH-related training award applications remaining stable over the last 5 years, yet increasing significantly in almost all other communities. Interestingly, within ICRH, differences were noted across its various research communities (Figure 5), with a decrease occurring in large areas such as cardiovascular and respiratory health, and an increase in smaller communities such as blood and sleep. Of greatest concern is the almost constant decrease in the number of postdoctoral fellows (the ones closest to beginning an independent scientific career) over the last seven years in cardiovascular and respiratory health, two areas of great disease burden. Collectively, these data would suggest difficulties in attracting, mentoring and/or retaining young researchers - a problem that appears to be particularly important for the two largest communities of ICRH.Figure 5: Evolution in number of funded trainees, by ICRH mandated field
(iii) Lower success rates and fewer applicants in Strategic Competitions, and inadequate balance across CIHR Themes?
Although the slower growth in total research funding in the ICRH community is largely due to a relative decrease in the number of trainees and researchers, data extracted from the CIHR database, suggests that ICRH investigators may have lower success rates at certain research competitions where the focus is, for example, on health systems/services and/or population/public health. Although ICRH investigators have had excellent success in large clinical research competitions, there is evidence that ICRH investigators have had lower success rates and significantly fewer researchers have applied (when compared to those from other CIHR communities) to other (non-OOGP) strategic grant competitions, particularly those involving multi-pillar, multi-disciplinary team research requiring KT and partnership funding. Indeed, from 2000 to 2010, the annual number of non-OOGP grant applications submitted by ICRH scientists decreased by 25%, while it increased 160% for CIHR as a whole. Furthermore, success rates at these competitions were consistently and significantly lower for ICRH applicants than the CIHR average (a difference that since 2006 has put ICRH scientists’ success rates for these grants at 6% to 12% below that of CIHR overall). Importantly, this suggests ICRH researchers are missing out on a number of funding opportunities and may indicate a need for more networking, both within and beyond the ICRH community.
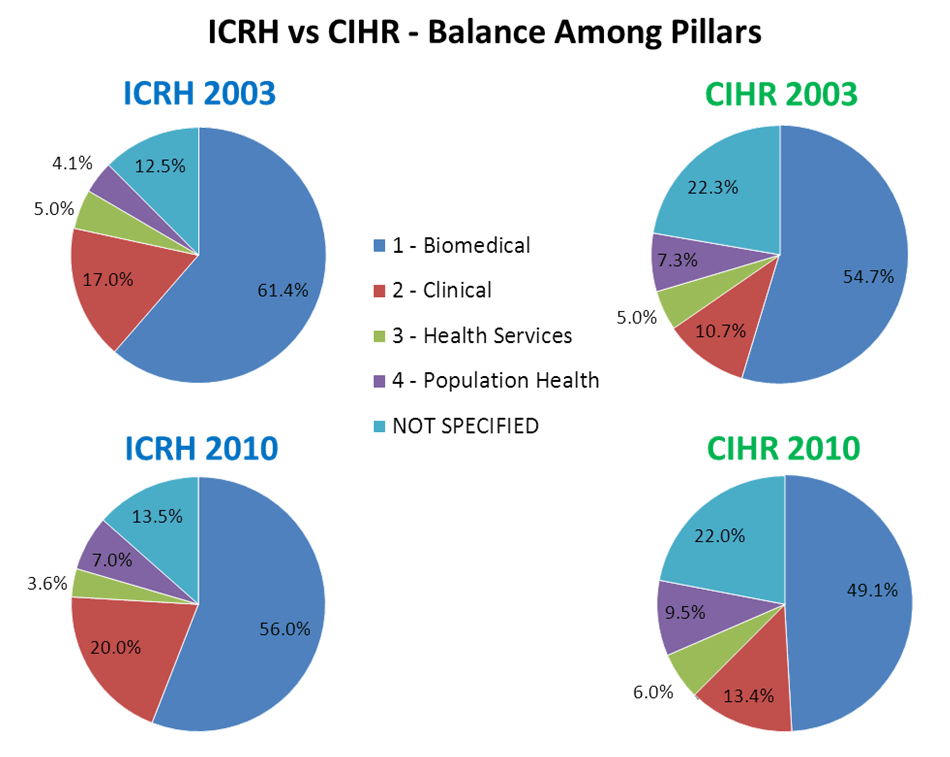
Analyses of CIHR data regarding the balance of funding according to the four CIHR themes (i.e., biomedical, clinical, health systems and services, and population and public health) in various ICRH communities, (i.e., cardiovascular and respiratory, blood, sleep,) seems to indicate a relative weakness and lack of growth in health systems/services and population/public health research (CIHR themes 3 and 4, respectively; Figure 6). The proportion of funding going to theme 3 in 2010-2011 among ICRH mandated fields represents slightly more than half compared to that observed for CIHR overall; the proportion of this funding has been decreasing since 2003 (from 5.0% to 3.6%) while that for theme 4 remains less than the proportion of funding observed for CIHR overall (7.0% vs. 9.45%), despite significant progress since 2003. Weaknesses across CIHR themes 3 and 4 could help explain the relative lack of funding of ICRH investigators in some strategic programs, particularly those with a focus on transfer of knowledge at a health systems and population level. Thus, there appears to be a need to develop capacity in areas related to health systems/services and population/public health.
Figure 6: Proportion of funding according to four CIHR themes
Paradoxically, despite relatively poor funding of clinical research within ICRH and CIHR as compared to other countries, investigators from the ICRH community are world leaders in clinical trials research. This is particularly true for investigators in the cardiovascular (Figure 7) and critical care fields. However, such successes remain fragile and require more adequate funding if they are to remain competitive.
Figure 7: Relative change in number of cardiovascular clinical trials publications since 1997 on an annual basis, comparing top 10 countries16
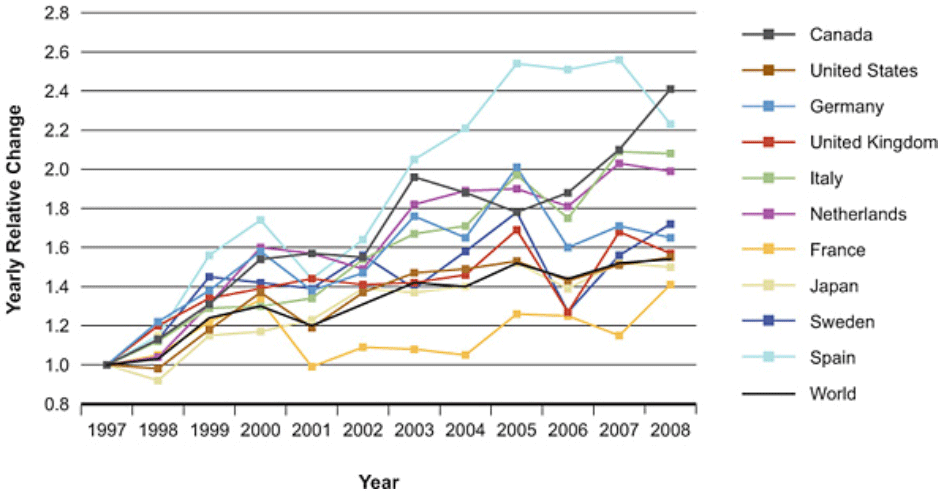
Data extracted by Observatoire des Sciences et Technologies from US National Library of Medicine Medical Subject Headings for 2000 to 2008, at request of CIHR.
4. ICRH Objectives and Strategic Priorities: 2013-2016
4.1 ICRH Objectives
In response to CIHR’s 10-year International Review panel, the latest ICRH External Review Panel, and the data mining and environmental scan presented above, ICRH identified the following 4 objectives, which align with CIHR’s strategic directions*:
- ICRH Objective 1: Increase the number and competitiveness of ICRH researchers in national and international grant competitions (*CIHR Strategic Directions 1 and 2)
- ICRH Objective 2: Achieve better balance across the four CIHR research themes in ICRH-relevant fields (*CIHR Strategic Directions 1 and 2)
- ICRH Objective 3: Enlarge the clinical trials activity in ICRH fields, particularly in respiratory health and stroke, and increase international collaborations in clinical trials (*CIHR Strategic Directions 1 and 2)
- ICRH Objective 4: Enhance transparency in priority-setting, planning, and decision-making (*CIHR Strategic Direction 3)
4.2 Strategic Priorities 2013-2016
To advance the above goals, ICRH will focus on the following four major priorities which will guide its programs and activities in the upcoming years:
- Enhance capacity, competitiveness, and impact through networking;
- Target training, mentoring and early career development to promote capacity building;
- Enhance opportunities for clinical, population health and health services research through cohort linkage and data enhancement; and
- Contribute to the advancement of relevant CIHR Roadmap Signature initiatives relevant to ICRH.
4.2. Priority 1: Enhance Capacity, Competitiveness, and Impact through Networking (*CIHR Strategic Directions 1 and 2)
A) Development of Complex Thematic and Cross-Cutting National Networks in Areas of Need and of Opportunity
In alignment with three recommendations from the ERP concerning capacity building, networking and the development of clinical trials, and consistent with the importance of aligning with CIHR’s largest Signature Initiative - the Strategy for Patient-Oriented Research (SPOR) - ICRH will focus one of its strategic initiatives around the development and support of national networks.
SPOR builds on Canada’s excellent profile in clinical research and will focus on improving health systems research in order to improve the efficacy of the health care system and the quality of health for Canadians. In order to achieve its objectives, SPOR is developing four major programs:
- Building the infrastructure for performing clinical research by:
- developing SUPPORT Units, a program developed in partnership with the Canadian provinces, but with national implications and
- developing SPOR comprehensive research Networks, developed in partnership with charities and other funding partners, in order to fill important gaps in clinical research;
- Training and career development programs focused on the expansion of the research community conducting patient-oriented research;
- Improving the clinical research environment as well as removing various impediments that obstruct valuable and productive clinical research in Canada; and
- Supporting best practices in health care.
ICRH’s strategic initiative focusing on the development of national networks differs in scope from that of the SPOR program as ICRH networks cut across all four CIHR research themes, focusing on all aspects of clinical translational research, from bringing discovery to patient care and back, as well as integration of population-level and/or health systems research. ICRH-supported networks will bring together unified groups of researchers in ICRH mandated fields to build a critical mass of outstanding technical and scientific expertise on a national scale, and provide research leadership in an effort to identify key knowledge gaps. These gaps will be addressed in a coherent fashion so as to maximize the potential impact of research on our understanding of disease and disease processes, on improved clinical practice, on the health of individuals and populations, and on the delivery of care. ICRH-supported networks will focus on central questions to direct pan-Canadian studies that are most relevant to Canadians. In addition, the networks will generate evidence and transfer it to the patient-care community.
Driven by scientific research leaders in Canada in a given domain, ICRH-supported networks are expected to contribute significantly to reversing the decline in trainees and young scientists. These networks will serve as hubs for attracting, mentoring, and training of emerging scientists, supporting early career development of young scientists, particularly in population health, health systems and services, and policy research. Linking together many of the best centers and teams in a given field, the networks will offer possibilities for tailored multidisciplinary, multi-site mentoring and training, attracting future trainees and young investigators eager to engage in networking as a means to develop their skills and enhance their knowledge-base. Importantly, these networks will enhance competitiveness by engaging the scientific community and partners (including non-profit organizations with expertise in end-user knowledge transfer, provincial research funding agencies and other government agencies, as well as industry) in large-scale national and international research programs. Networks will also offer opportunities for developing clinical trials, particularly in areas of need such as in stroke and respiratory health. The ICRH Emerging Networks RFA was launched in the summer of 2012 with funding that started in October 2013.
Although ICRH networks can span broader range of patient-oriented research as compared to the SPOR Networks (i.e., going from bench-to-bedside research and extending to health systems and population health), ICRH and SPOR networks are expected to share many common characteristics. Thus, in addition to complementing the SPOR program, it is anticipated that, in the future, some of the ICRH-supported networks will compete to become SPOR Networks. If successful, ICRH’s funding for these networks would be applied to support these new SPOR networks.
Based on feedback from the External Review Panel (International Review) and identified gaps and opportunities, the three major areas targeted by ICRH for Network development are:
- A National Respiratory Network. According to the 2012 report produced by The Council of Canadian Academies17, Canada is well regarded internationally for its research in the respiratory system sub-field, being placed fourth in the world in terms of productivity and impact in this research area. The development of a Canadian respiratory network, through the ICRH Emerging Networks RFA, will build on this Canadian strength. In addition, the new program will answer a long term wish of the respiratory community and its partners to develop a formal national network in a field with an important and growing disease burden and equally important knowledge gaps. Considering the global trend towards networking, without this development, it is unlikely that the Canadian community will be able to maintain its enviable position. This network would also address two of the specific recommendations of the ERP, concerning the development of networks and the development of a clinical trials capacity in this field.
- National Vascular Network. In early 2011, this large and disparate community had already started to come together with the expressed goal of developing a National Vascular Network. Taking advantage of the groundwork initiated by this community and the considerable potential of their collaborations, ICRH chose to support the development of a Network in this area as one of its priorities. Funding of this community will provide an opportunity for ICRH to support this community in their pursuit towards addressing key issues that have immense impact on several organ end-points including heart, brain, kidney, eyes, etc.
- A National Stroke Prevention through Atrial Fibrillation Clinical Trials Network. Canada has a stroke Networks of Centres of Excellence (NCE) – the Canadian Stroke Network - that has successfully changed the way strokes are being considered by the public and treated by the health care system. The proposed ICRH network I an extension of this NCE, but will focus on stroke prevention clinical trials research, an area that was not targeted as a priority by the Canadian Stroke Network. In this way, ICRH will leverage the expertise of the strong but financially fragile stroke clinical trials community, and be complementary to what has been accomplished by the stroke NCE.
B) Establishment of Focused Community Development Programs
The ICRH research community has a number of very strong, focused, and successful research communities in other research fields not mentioned above, including critical care, stroke treatment and recovery clinical trials, sleep & circadian rhythms, and blood diseases. To date, these four research communities have successfully conducted major practice-altering research without significant outside strategic funding. This is largely due to the exceptional circumstances under which they were developed and the collective strategy that drives their success. Presently however, these groups are at a crossroads; they can either continue, with difficulty, as they are today, or optimize and expand their programs to include additional training and knowledge transfer activities. Recognizing the strength of these ICRH communities, and based on ERP feedback (International Review), ICRH will target these four focused areas for the establishment of community development programs in: critical care, stroke treatment and recovery clinical trials, sleep & circadian rhythms, and blood disease research.
- National Critical Care Program. The critical care trials community in Canada is an extraordinary national asset composed of a broad and vibrant research community of scientists, clinicians, and trainees, working together in a field where quality of care and effectiveness research can be applied in life or death situations to improve efficacy and reduce costs, while improving survival and health prospects of the populations. Notably, this group does not benefit from CIHR or ICRH strategic funding. It has become apparent that for these Canadian researchers to sustain their international success and leadership, they must be supported as a community. The funding of a targeted program in this field would allow much faster implementation of pilot studies, thus permitting greater development of evidence to guide the therapy of patients in the critical care setting. It would also facilitate the enhancement of the training and of knowledge transfer activities of the group, an area where best practices have already been developed.
- National Stroke Treatment and Recovery Clinical Trials Program. In Canada, the community of investigators active in the field of diagnosis, treatment, and recovery from acute stroke constitutes a vibrant group that consists of scientists and clinicians working in major stroke and stroke recovery units across the country. Unfortunately, despite its excellence in designing and/or conducting research projects and clinical trials, this community does not have the resources or organized infrastructure to optimally broaden the scope of its research activities as well as optimally develop a broader approach to patient-oriented research. Through a targeted stroke treatment and recovery community development program, ICRH anticipates advancing the capacity, competitiveness, and impact of research conducted in Canada by this community.
- National Sleep & Circadian Rhythm Program. In June 2009, ICRH and partners launched two Sleep and Circadian Rhythms programs - Operating Grants and Teams Grants - which addressed one of ICRH’s research priorities (ICRH Strategic Plan 2006-2010). Notably, during the Institute’s review, the ERP commented that sleep research is an area of strength in Canada that could benefit from the development of a national consortium. Based on this feedback and building on our past initiatives, ICRH has chosen to focus on supporting a large scale national program in this area to enable the sleep & circadian rhythm community in Canada to take into consideration more multi-disciplinary and multi-thematic approaches, collaborate more effectively, and compete successfully for additional national and international funding.
- National Blood Disease Program. Canadian researchers working in the area of coagulation have been at the cutting edge of defining best practices for the use of anticoagulants in improving patient outcomes in a large number of clinical situations. ICRH plans on building on this strong tradition and supporting the expansion of the existing interests of this community in knowledge transfer, patient engagement, training and mentoring, and impact of health systems research.
C) Support of Ongoing International Clinical Trials Networks
According to the 2012 report produced by the Council of Canadian Academies17, Canada’s level of international collaboration is particularly high in areas related to clinical medicine. Building on this strength, ICRH, since 2003, has worked closely with the National Heart, Lung and Blood Institute (NHLBI) of the NIH to support two large Canada-US networks: the Resuscitation Outcomes Consortium (ROC) and the Cardiothoracic Surgical Network (CTSN). The ROC is a network conducting clinical research that has improved the way resuscitation is performed around the world. The second network, the CTSN, is the leading cardiothoracic research network in the world. In support of CIHR’s vision – enhance patient-oriented care and improve health outcomes - and the great contributions of Canadian researchers to the success of these two networks, ICRH intends to continue funding these Networks in the upcoming years.
4.2.2 Priority 2: Training, Mentoring and Early Career Development to Promote Capacity Building (*CIHR Strategic Directions 1)
As shown above, recent data indicates that the growth of funding within ICRH’s mandated research areas has been slower than in all other areas at CIHR. This is particularly problematic in the cardiovascular and respiratory areas where funding is on the decline. Analyses of the situation suggests this decline is due, at least in part, to comparatively fewer new investigators entering these fields, a problem that appears to stem from an important reduction in the number of senior trainees (postdoctoral fellows), in cardiovascular and respiratory health, and a severe shortage of graduate students in most of the ICRH-mandated fields. A second problem is one of imbalance between research themes, with a particularly severe shortage of investigators in health services and policy research as well as in population and public health (CIHR themes 3 and 4).
According to the Council of Canadian Academies 2012 report17, Canada has the largest number of post-secondary graduates in the Organization for Economic Co-operation and Development (OECD). Thus, while there is a strong base from which to build, this is not translated into large numbers of doctoral graduates who could contribute to science and technology in this country. Moreover, the report suggested Canada lags behind some other countries in regards to the number of researchers, and in the training of the next generation of researchers. Thus, CIHR has identified training and career development as an area that needs greater attention. As such, CIHR is now in the process of developing recommendations and new programs to advance these areas of need. An ICRH IAB task force, enriched by membership from ICRH’s close partners, has also studied this problem and has developed recommendations to address this challenge, recommendations that are consistent with those recommended by the SPOR training, mentoring and career development working group led by Norm Rosenblum. ICRH will also continue working with partners and various stakeholders to develop a joint, comprehensive strategy that directly aligns with elements of partner-led programs. To ensure this strategy is comprehensive, it will also include commitments from recruiting institutions and partner organizations which will address the most critical factors for successful career launch (regarding salary support, structured mentoring, protected research time, adequate space and equipment support, start-up operating funds, and a clear academic career perspective). ICRH is particularly interested in supporting initiatives that will enhance training, mentoring and career development for ICRH researchers working in areas relevant to CIHR’s themes 3 and 4.
ICRH together with its many partners anticipates establishing an effective training, mentoring and early career development strategy, that will focus on those factors identified as being critical for effective training/mentoring as well as for early success (i.e. within the first three years) in a research career. It is our hope that such a strategy will, in turn, attract senior trainees and improve the application and success rates of new investigators.
4.2.3 Priority 3: Enhance opportunities for clinical, population health, and health services research through cohort linkage and data enhancement (*CIHR Strategic Directions 1 and 2)
The Canadian Heart Health Strategy18 recommended that priority be given to the development of a cardiovascular cohort to enhance Canada’s capacity to advance knowledge on the relative role of various risk factors, including those related to environment and community as well as those related to lifestyle and biological determinants of cardiovascular disease. Improving our understanding of the complex interplay between these risks factors is critical, particularly given the increased prevalence of many of these cardiovascular risk factors for acute and chronic cardiovascular diseases.
Over the years, a number of Canadian health-scientists, groups, teams, and networks have developed a range of cohorts, each with its own specific focus (e.g., for cardiovascular disease, diabetes, respiratory diseases, cancer, children, etc.). Such cohorts were funded, at least in part, with public funds. Unfortunately, most of these cohorts were developed in abstraction of each other. As such, these cohorts are frequently underutilized, seldom shared with scientists in other institutions, and almost never with those in other fields/disciplines despite collecting data on several similar risk factors. Despite the significant efforts and cost involved in developing a cohort, existing Canadian cohorts constitute a relatively untapped resource that can provide researchers an opportunity to compare, coordinate and extrapolate findings with that of similar health data at a national and international level.
The goal of this ICRH strategic priority is to develop a program that will help harmonize and enhance Canadian cohorts through the linkage of existing cohorts and enhancement of their data in such a way as to allow the development of more effective interventions at the individual and community levels. This undertaking will provide Canadian scientists, particularly in clinical research, health systems and population health research, with a formidable and unique asset that could boost knowledge development and knowledge translation at a fraction of the cost of developing new cohorts. Moreover, harmonization and linkage among cohorts will accelerate the capture of the benefits of health research and, thus, place Canada at the forefront internationally.
Along with CIHR and its other Institutes, ICRH will work to allow disparate and multidisciplinary communities to first work together towards common goals, bridging gaps and identify ways for sharing and harmonizing population-relevant data sets. The linkage and enhancement of multiple existing Canadian cohorts will enable Canada to improve population-based research and design both community-based and patient-specific prevention and intervention programs. In addition, this initiative will greatly enhance the potential for health and health systems research in Canada by creating a formidable pool of population-based data linked to uniquely powerful administrative databases, permitting scientists and health-care professionals to follow outcomes and use of health services. Cohort linkage and data enhancement will also directly assist in gathering and analyzing important, yet sparse, data relating to Canada’s Aboriginal Peoples and other vulnerable populations. Through the emerging Environments & Health RSI, ICRH will strive to create opportunities to link a wide array of potential environmental health determinants to large, well-characterized cohorts in order to create a national resource for conducting environmental health research in Canada. Finally, by addressing data enhancement and storage, as well as issues pertaining to access policies, research ethics board (REB) assessment, and re-consent issues, this priority will pave the way for improved organizational excellence and create opportunities for knowledge expansion in research on ethics.
4.2.4 Priority 4: Contribute to the advancement of relevant CIHR Roadmap Signature Initiatives (*CIHR Strategic Directions 2)
CIHR has developed eight large Roadmap Signature Initiatives to support its objectives. Of these the largest, and the one with which ICRH aligns most closely, is the Strategy for Patient-Oriented Research (SPOR). However, as outlined below, ICRH is directly or indirectly involved with and also supports most other Roadmap Signature Initiatives.
A) Inflammation in Chronic Disease
-
Health Challenges in Chronic Inflammation Initiative. Inflammation is a physiological process that normally helps fight infection and aids in tissue repair. Dysfunctional inflammatory responses, however, contribute to the development and progression of several common chronic diseases including asthma, chronic obstructive pulmonary disease (COPD), and chronic bronchitis – key research areas under the ICRH mandate. Inflammation also contributes to the development and progression of a number of other diseases such as cardiovascular disease, arthritis, diabetes, neurodegeneration, neurological and neuropsychiatric disorders, and cancer. These and other diseases with underlying inflammatory pathology are placing a burden on health care costs and human suffering across the globe. Currently, our understanding of how chronic inflammation is involved in the development and progression of disease remains limited, and the remaining scientific challenges are enormous.
The aim of this Roadmap Signature Initiative is to identify commonalities between diseases in which inflammation plays a role. This approach may hold the potential for understanding chronic inflammatory physiopathology more accurately, permitting earlier diagnosis, and more effective treatment alternatives. To help address these goals, which also directly relate to one of ICRH’s former priorities (2006-2010 Strategic Plan), the Institute will provide funding for applications that address research on inflammation as related to respiratory health.
-
Transplantation Research Initiative. Closely related to the chronic inflammation signature initiative, and involving many of the same stakeholders, is an initiative focusing on transplantation, which in itself is largely influenced by inflammation. As ICRH’s research community identified transplantation as one of its research priorities (ICRH Strategic Plan 2006-2010), ICRH has worked with the CIHR-Institute of Infection and Immunity and other partners to establish a national transplantation consortium. By bringing together the country’s expertise in this field, sharing platforms and resources, and creating transplant teams and networks, this initiative aims to transform transplantation research in Canada, leading to an increase in the quality and the quantity of donor organs, and improved long-term health outcomes for transplant patients. As this community and partners were ready for such an initiative at an early stage of this strategic plan, the Canadian National Transplant Research Program has now been launched and has been operating since 2012 with the support of ICRH funding, subsequent to an RFA and peer review process.
B) Personalized Medicine
According to Canadian science and technology experts17, personalized medicine is one of the top emerging science and technology areas where Canada is positioned to be a global leader. Notably, the topic of ‘biomarkers for chronic disease’ has been one of ICRH’s top priorities since 2006.
To further support the discovery, validation, and translation of biomarkers as they relate to the ICRH research areas, the Institute joined the Genomics and Personalized Health program – a component of the Personalized Medicine Signature Initiative. ICRH has committed specific funds to support projects that directly align with any of the three ICRH Emerging Networks; it is our hope that the ICRH-relevant team(s) supported through the Genomics and Personalized Health competition will establish strong links and collaborations with the new ICRH Emerging Network(s), some of which are predicted to have a strong biomarkers component to their research program.
C) International Collaborative Research Strategy for Alzheimer's Disease
Vascular disease plays as important of a role, if not a more important role, in the development of cognitive impairment than does Alzheimer’s disease19 and given that ‘aging and the cardio-respiratory system’ has been identified as a research priority (ICRH 2006-2010 Strategic Plan), ICRH will work closely with the Institute of Aging to develop this initiative that will bring together a number of groups with expertise in Alzheimer’s disease. ICRH will contribute funds to support the development of an integrated consortium-based research program that will incorporate the appropriate vascular elements (a mandate of ICRH) and their role in the development of cognitive impairment.
D) Pathways to Health Equity for Aboriginal Peoples
ICRH, through its cohort linkage and data enhancement initiative (priority three), seeks to develop, in collaboration with CIHR’s Institute of Aboriginal Peoples’ Health (IAPH), an aboriginal cohort consisting of approximately two thousand reserve-based individuals. As part of this initiative, ICRH will work with its community, the Heart and Stroke Foundation, and an expert committee from IAPH to support the development of this cohort that will aim at thoroughly phenotyping, including contextual phenotyping, of these individuals. This undertaking will create an important resource that will be used to conceive and evaluate programs designed to improve the health and health care of these communities. Importantly, the data collected through the cohort could be of great value to researchers and programs that will be developed through the CIHR Pathways to Health Equity for Aboriginal Peoples’ Signature Initiative.
E) Environments and Health
In partnership with CIHR Institutes of Population and Public Health; Infection and Immunity; Human Development, Child and Youth Health; and Nutrition, Metabolism and Diabetes, ICRH will contribute to the development of the Environments and Health Roadmap Signature Initiative. This program will examine the effects of physical (natural and built), chemical, social and cultural environments and their interactions on health and disease. For ICRH, topics such as air pollution, chemical exposure, and built environment among others are particularly relevant to respiratory and cardiovascular health. Aligning with the cohort linkage and data enhancement research priority, we will support efforts that will focus on enriching existing cohorts with new generic and specific environmental data. Ultimately, this work will allow researchers to better appreciate how different environments impact health as well as improve understanding of how to optimize inter-sectorial systems so as to prevent, reduce, mitigate or enhance resilience to environmental threats.
5. Conclusions
As ICRH operationalizes its strategic plan, it will attempt to reverse the progressive relative loss of research capacity in many of its communities. The Institute proposes to achieve this goal through four major priorities. The first will focus on the development of a series of thematic Networks and Community Development Programs that will bring together the country’s scientific expertise to address knowledge gaps, create opportunities for leveraging resources through partnerships, and generate unique training/mentoring opportunities. These programs will enable ICRH to focus on its second priority – improve training/mentoring and support early career development – and will address an urgent need to expand both the number and scope of early career investigators working within ICRH mandated research areas. Such a strategy should ensure Canada remains able to adequately address current and future health care concerns. Thirdly, ICRH’s priority to foster cohort linkages and data enhancement will involve coordination among multiple CIHR Institutes and partners. It is our hope that this initiative will enable ICRH to attract health systems and population health researchers to areas relevant to the Institute’s mandate as well as increase the capacity for meaningful health-related environmental research in Canada. ICRH’s fourth priority - participation in and contribution to various CIHR Roadmap Signature Initiatives - will create multiple opportunities for our community to reach out and partner with other strong teams and groups with similar interests within the Canadian community. Notably, patient engagement will be an important priority that will serve as one of the major building blocks of all ICRH clinically related initiatives. Active engagement of patients will strengthen our communities and promote long-term transformational change to the benefit of all Canadians.
References
- Footnote 1
-
CIHR Act 2000; February 13, 2013 – Page 3.
- Footnote 2
- Footnote 3
-
Organisation for Economic Co-operation and Development (OECD) – Health data 2012.
- Footnote 4
-
Moving Forward – CIHR Performance Across the Spectrum: From Research Investments to Knowledge Translation. CIHR Corporate Publication 2011–12–09.
- Footnote 5
-
Morgan S, Grootendorst P, Lexchin J, Cummingham C, Greyson D. The cost of drug development: A Systematic Review. Health Policy 2011; 100:4-17.
- Footnote 6
-
Berwick DM. Disseminating innovation in Health Care. JAMA 2003; 289(15):1969–1975.
- Footnote 7
-
Herzlinger RE. Why innovation in Health Care is so bard - Big Picture. Harv. Bus. Rev. On point 2006 (May):1-10.
- Footnote 8
-
National Institute for Health Research UK. 2011 (Annual Report).
- Footnote 9
-
Public Health Agency of Canada – Data from the Economic Burden of Illness in Canada 2000.
- Footnote 10
-
Based on the total cost illness of $147,9 billion. Expenditures for care in other institutions and additional direct health expenditures are not included.
- Footnote 11
-
Direct costs include hospitals, drugs and physician.
- Footnote 12
-
Indirect costs include mortality, long-term disability and short-term disability.
- Footnote 13
-
Lenfant C. Clinical Research to Clinical Practice-Lost in Translation. NEJM 2003; 349:868-874.
- Footnote 14
-
Murray CJL, Lopez AD. Alternative Projections of Mortality and Disability by Cause 1990–2020. Global Burden of Disease Study. Lancet 1997; 349:1498–1504.
- Footnote 15
-
International Review of the Canadian Institutes of Health Research – Expert Review Team Report for the ICRH – S. Holgate – 2011 (February).
- Footnote 16
-
CIHR Institute of Circulatory and Respiratory Health – International Assessment for 2011- International Review – Page 12.
- Footnote 17
-
The Council of Canada Academies: The State of Sciences and Technology in Canada 2012.
- Footnote 18
-
Canadian Heart Health Strategy and Action Plan – Building a Heart Healthy Canada – Health Canada 2009 (February).
- Footnote 19
-
Kovacic JC, Fuster V. Artherosclerotic risk factors, vascular cognitive impairment and Alzheimer disease. Mt Sinai J Med 2012;79(6):664-673.
- Date modified: