Evaluation of the Institute of Neurosciences, Mental Health and Addiction (INMHA)
Report of INMHA Evaluation Panel
November 2016
At the Canadian Institutes of Health Research (CIHR), we know that research has the power to change lives. As Canada's health research investment agency, we collaborate with partners and researchers to support the discoveries and innovations that improve our health and strengthen our health care system.
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
This publication was produced by the Canadian Institutes of Health Research. The views expressed herein do not necessarily reflect those of the Canadian Institutes of Health Research.
INMHA Evaluation Panel: Dr. Yves De Koninck (Chair), Deanna Groetzinger, Dr. David Kaplan, Dr. Serge Rivest, and Dr. Glenda MacQueen
Acknowledgements
Thanks to all participants in this evaluation –survey respondents, interview and case study participants – and to Program Evaluation and Beyond, Circum Network Inc., and the Observatoire des sciences et des technologies for data collection and analysis.
Additional thanks to the INMHA CIHR Evaluation Team: Michael Goodyer, Abigail Forson, David Peckham, and Hayat Ghazal.
And special thanks to the CIHR-INMHA Scientific Director Dr. Anthony G. Phillips, and Dr. Eric Marcotte, Associate Director, INMHA.
For more information and to obtain copies, please contact Evaluation@cihr-irsc.gc.ca
Table of Contents
- Observations & Recommendations
- Evaluation Overview and Key Findings
- Overview
- Key Findings
- Relevance
- Ongoing relevance of support to INMHA research
- Appropriateness of Current INMHA mandate
- Changes to Institute Name
- Funding landscape
- Emergence of New Players in INMHA Ecosystem
- Transformative Impact
- Support to Innovative Research and Advancing Knowledge
- Contribution to Building the Capacity of the Health Research Enterprise
- Contribution to achieving broader health, economic and social impacts
- Convener and Catalyst
- Operational Effectiveness
- Relevance
- References
- Appendix 1: Overview Data Sources and Methods
- Appendix 2: Figures and Tables
- Figure 1: Partner Contributions to INMHA funded research 2000-07- 2008-14
- Figure 2: CIHR Investment in INMHA mandate area, by type, 2000-2014
- Figure 3: INMHA Institute Strategic Budget, 2009-2015
- Figure 4: CIHR spending in INMHA mandate areas, 2000-2014
- Figure 5: Proportion of world papers and of top 10% most cited papers, Canada, 2000-2014
- Figure 6: Canada in comparison to other Countries Specialized Index (SI) and Average Relative Citations (ARC)
- Table 1: Top 10 investors in INMHA’s mandate
- Table 2: INMHA strategic investment priorities, as abstracted from 2001-06, 2007-11 and 2012-17 Strategic Plans
Observations & Recommendations
Overview of Institute of Neurosciences, Mental Health and Addiction (INMHA)
As one of the 13 CIHR Institutes, the Institute of Neurosciences, Mental Health and Addiction (INMHA) has a mandate to support research that enhances knowledge of the brain, mental health, neurological health, vision, hearing and cognitive functioning.
To achieve this mandate, INMHA supports innovative research that provides new knowledge of the biological and socio-cultural processes underlying cognition and emotion in the context for good health, mental ill-health and addiction.
INMHA’s overall goal is to reduce the burden of brain illnesses through the translation of these new insights into brain function, coupled with prevention strategies and better diagnosis and treatment strategies.
Overview of the Evaluation
The evaluation of INMHA was conducted by CIHR as part of a rolling review of the mandate and performance of CIHR Institutes. The evaluation assessed the relevance and performance of INMHA to inform decisions regarding the role and functioning of the Institute. The evaluation was overseen by an Institute Evaluation Panel comprised of experts in INMHA’s mandate areas and conducted by CIHR Evaluation Unit and external evaluation professionals.
Should INMHA be amended, merged or terminated?
Context
The wide mandate of INMHA, encompassing neurosciences, mental health and addiction, represents a highly important area of science for Canada and Canadians.
The brain is now regarded as the ‘last frontier’ in basic health research, where many discoveries continue to be and still need to be made. This is highlighted in major scientific venues,Footnote 1 popular science articles,Footnote 2 and internationalFootnote 3 and Canadian studies and policy initiatives such as the 2007 Canadian Institute for Health Information report: The Burden of Neurological Diseases, Disorders and Injuries in Canada.
Within the domain of mental health research, a key change in the landscape has been an increased recognition of the burden of mental illness and prioritization of mental illness as an area in need of greater knowledge. Similarly, in addictions research, there is an increased recognition of population burden, especially regarding emerging epidemics in prescription opiate abuse and a changing policy environment for prescription drug management and legalization of marijuana.
The burden of disease perspective highlights the immense social and economic burdens of neuropsychiatric disorders. The impact on the Canadian economy is significant; when the direct and indirect costs of neurological disorders and mental health are tallied, these account for $61B per year.Footnote 4
Scientific landscape
Canada has ongoing and increasing national strength in the area of neurosciences, mental health and addiction research. This strength reflects the major commitments and investments made by Canada in these research areas to build a strong research community.
Bibliometric data from the evaluation illustrate that Canada’s rank in terms of the share of world papers in addiction (4th), mental health (5th), neurosciences (5th) and senses (6th) are above Canada’s overall ranking in all fields of health research (seventh or eighth depending on the year). Canada’s rankings in terms of impact, as measured by average of relative citations (ARC), are as follows: addiction (7th), mental health (5th), neurosciences (3rd) and senses (5th).
In terms of specializationFootnote 5, the areas of neuroscience and the senses represent clear strengths for Canada. Canada is the most specialized country in neurosciences, second in senses, and fourth in mental health and addictions.
The panel recognized that CIHR, which since its inception has been the major funder of the neurosciences in Canada, has been largely responsible for the impressive ranking of Canada in the neurosciences, mental health and addiction and senses research fields.
Funding Landscape
Research funded by CIHR in the INMHA mandate area constitutes a significant proportion of total CIHR investments. On average, investments in research relating to INMHA’s mandate represented 24% of total CIHR investments over the period from 2000-01 to 2014-15. Total investments in 2014-15 in this area were $229.6M, primarily through investigator-initiated research (e.g., Open Operating Grant Program). Only the Institute of Genetics and the Institute of Infection and Immunity have a higher proportion of investments in their mandate areas at 34% and 26% respectively.
In 2014-15, CIHR provided funding support to a total of 11,355 health researchers and trainees, of whom 3,624 (32%) were in INMHA’s mandate areas.
The panel has noted considerable evolution in the national funding landscape for research in these areas. In the last ten years, newly funded federal organizations have emerged within INMHA’s research space, with particularly significant investments through the Brain Canada Foundation and Mental Health Commission of Canada (MHCC).
In 2011, the Government of Canada announced the establishment of the Canada Brain Research Fund (CBRF) with a $100M commitment to encourage Canadians to increase their support of brain research, and maximize the impact and efficiency of those investments.Footnote 6 An additional $20M was allocated in the 2016 budget. The federal government also committed $130M over 10 years in 2007 to establish the MHCC, an arm's length, not-for profit organization designed to improve health and social outcomes for people and their families living with mental illness.Footnote 7
Achieving its mandate
It is clear that the INMHA Scientific Director and his leadership are very highly regarded and this is acknowledged by the panel. The Scientific Director was cited as particularly gifted in anticipating changes in the research landscape and responding to these, highly skilled at facilitating conversations and collaborations, and effectively implementing strategic and operational plans.
A key success of the Institute has been the creation and fostering of partnerships with researchers, knowledge users and funders. INMHA’s partnerships have resulted in an increased leveraging of funding from $7.9M for the period 2001-02 to 2007-08 to $31.9M for the 2008-09 to 2014-15 period. Notably, international partner contributions to INMHA funded research increased sharply from $1M to $17.5M (17-fold increase), not-for-profit partner contributions increased from 730K to $8.3M, and for-profit partner contributions increased from $1.2M to $1.8M over these two periods.
It is clear to the panel that INMHA has supported excellent, innovative and impactful research. There is corroboration of this view in the survey of researchers: 58% of researchers agreed that INMHA funding supported innovative ideas in their research.
The panel has seen that INMHA has played a key role in developing international and cross-national research collaboration efforts. These have provided opportunities for Canadian researchers to participate in key global fora, with the International Initiative for Traumatic Brain Injury Research (InTBIR) and International Human Epigenome Consortium (IHEC) as key examples.
Working closely with the Institute of Genetics and the Institute of Cancer Research, INMHA led the development of the Canadian Epigenetics, Environment and Health Research Consortium (CEEHRC) – a CIHR Signature Initiative aimed at ensuring that Canada plays a leadership role in the field of epigenetics. INMHA’s leadership has been key to creating external partnerships, such as with Japan for a dedicated Epigenetics of Stem Cells team grant program. Through this Signature Initiative, CIHR has been a founding member of IHEC—a >$130M global consortium.
As the strategic lead on the Canada-China Joint Health Research Initiative (CCJHRI), INMHA worked closely with other CIHR Institutes to establish a strong working relationship with the National Natural Science Foundation of China (NSFC) which has resulted in the ‘twinning’ of 135 Canadian labs with 135 Chinese partners. The initiative was formally evaluated and found to be mutually beneficial to both Canadian and Chinese researchers paving the way for a third phase of this partnership.
INMHA provided major oversight for CIHR’s Regenerative Medicine and Nanomedicine Initiative (RMNI), an $88M project that improved collaboration with Natural Sciences and Engineering Research Council of Canada (NSERC) laid the ground work for nanotechnology and regenerative medicine in Canada. The evaluation of RMNI, completed in 2013, concluded that the initiative made a significant contribution to the Canadian health research enterprise in its targeted fields since its launch in 2004.
INMHA is also supporting research to improve health systems and services in the area of mental health and senses. A recent evaluation of INMHA’s contributions and support to the SPOR Network in Youth and Adolescent Mental Health - ACCESS Open Minds showed that the network addressed a key area of gap in youth mental health.
While INMHA has increasingly focused its strategic efforts in a few key areas with the goal of enhancing Canada’s competitiveness in those areas, the resulting initiatives (epigenetics, TBI, for example) only engage small sectors of the research community. The Scientific Director has recognized this, and in the past year, has initiated conversations and workshops with national neuroscience research leaders, the Brain Canada Foundation, Canadian Institute for Advanced Research (CIFAR), and the leaders of several of the neuroscience-focused grants awarded by the Canada First Excellence Research Fund to develop a national brain research initiative which will benefit the maximum number of researchers in the neuroscience community. This demonstrates that INMHA and the Scientific Director play important leadership roles in bringing the disparate neuroscience research community together to develop innovative, novel, and multidisciplinary cross-Canada initiatives. Furthermore, the Scientific Director has admirably and for the first time effectively engaged several of the different organizations funded by the federal government that focus on neuroscience, including CBRF and NeuroDevNet, as partners with CIHR in a common national initiative.
Conclusion
The panel believes that there is a need for a strong CIHR voice in the area of neurosciences, mental health and addiction research. INMHA has demonstrated that it has played this role during the period under review.
The growth and evolution of the landscape of international brain research has shown it to be critically important that CIHR has a strong and credible presence. The recent emergence of brain initiatives across the world, such as the B.R.A.I.N. Initiative in the United States, the Human Brain Project and the China Brain Project, underscores the importance of the Institute as an advocate for Canadian neuroscience.
CIHR is the largest funder of neurosciences, mental health and addictions research in Canada.
Under the current Scientific Director, INMHA has demonstrated the importance of having an advocate who can facilitate and establish strategic priorities and collaborate and leverage funding nationally and internationally.
Without an Institute focused on this area, it would be difficult for CIHR to effectively fulfill the role of national advocate around international tables with a credible voice and understanding of the research fields involved.
The panel concludes that given the Institute’s already broad mandate, the merging of INMHA with other Institutes would have a negative impact on its ability to effectively convene and advocate for these research communities. Further, INMHA has demonstrated an effective track record in collaborating with other Institutes, particularly in research areas where there is cross-over.
Recommendation 1: The Panel recommends that INMHA should be retained and not be amended, merged or terminated
Whether INMHA’s mandate should be changed?
Panel perspectives on mandate
INMHA has a broad mandate, which poses a challenge for the Scientific Director and Institute to work effectively with the various communities. In light of this, there is a tension between a potential fragmentation or separation into components and an ongoing integration within the mandate.
The separation of INMHA’s mandate into smaller components could allow for the less funded areas such as addictions and mental health research to be more adequately supported. Here, the comparisons between INMHA and the National Institutes of Health (NIH) in the US were generally positive, in that the NIH approach tends to the fragmentation and “siloing” of neuroscience versus mental health versus addictions research. The advantage of integration under a larger umbrella of scientific inquiry about the brainunder the current INMHA structure is that all components potentially benefit from interdisciplinary cross-fertilization.
To narrow the mandate or break into components would go against a positive trend of increasing growth and integration of neuroscience, mental health and addiction within Canada and internationally (e.g., as does the Society for Neuroscience). Further, it would also send a message to the community that CIHR does not see these fields as integrated. It is the view of the panel that the Institute should have an integrative role in its fields of research and continue to aim to attain balance among the mandate areas.
Institute name
The panel believes that there is an opportunity to move to a more integrative and simpler name for the Institute.
The bibliometric analysis indicates an increasing homogeneity in the performance of different areas of research within INMHA’s mandate. This is despite a relative dominance of neuroscience compared to mental health and addiction in both investments and reported impacts.
A simpler, broader Institute name would reflect the wider evolution towards ‘brain science’ as well as address all domains, which the current name does not cover. Based on this, the panel suggests that CIHR and the Institute should consider a change to a name that better represents a common focus on the brain. It is understood that a name change would need to be undertaken in consultation with the community before coming to a consensus on a new name.
Potential names the panel discussed for consideration included the following:
- Institute of Brain Research;
- Institute of Brain and Mental Health Research; and
- Institute for Brain Health Research.
Role of Institute
The panel recognizes that the role of a CIHR Institute is different from that of NIH. The primary role of a CIHR Institute is as a convenor and catalyst to bring communities together and establish partnerships.
Throughout the evaluation, the panel considered the wider question of the evolving role of Institutes within CIHR. In particular, the panel discussed the changes resulting from Institutes Modernization in 2014-15, whereby half of CIHR Institutes’ research budget ($55.9M per year out of $111.8M per year) is now invested in the Roadmap Accelerator Fund (RAF) to support multi-Institute and multidisciplinary initiatives aligned with the priorities set out in CIHR’s five-year strategic plan, Health Research Roadmap II.
The demonstrated success of the Institute is almost entirely based on the model, resources and activities of the past 14 years prior to the Institutes Modernization. As a result, the nature and extent of these achievements may be endangered under the new model and, as such, should be monitored. For instance, the emergence of large international brain research initiatives will require significant investment for Canada to continue to play a lead role globally. This will require that the Scientific Director have access to considerably more strategic funds and the ability to use those funds at their discretion with considerable input and advice from the research community. This is the model used by the NIH to successfully establish the NIH national B.R.A.I.N. initiative.
While collaboration on cross-cutting initiatives between Institutes and areas of research are highly important, it is the panel’s view that there is a trade-off in terms of freedom of action, ability to partner on or lead initiatives, and address the key needs of the community.
In the case of INMHA, this creates challenges in how a Scientific Director can partner with other Institutes and organizations and focus on the issues most relevant to the INMHA community. If the Scientific Director has only very limited means at their disposal to make investments, their ability to meaningfully act on and invest in opportunities of importance to INMHA as well as bring others to the table is diminished.
The panel is concerned that INMHA’s current budget for funding research will make it difficult for it to fulfill its broad mandate. If the Institute is to launch new impactful, broad-based and visionary programs, more funding and more flexibility is needed, with a greater emphasis on the discretion of the Scientific Director to act.
Finally, the panel recognized that the elimination of the Institute-specific Advisory Boards has severely compromised the ability of INMHA to recognize and develop, and to achieve consensus on strategic initiatives. The Institute-specific Advisory Boards provided an expert panel to advise and inform the Director, and most importantly, to provide a bidirectional communication portal between the research community and INMHA. Without an Institute-specific Advisory Boards, there is both a loss of expertise available to the Director and a perception issue whereby the community does not know how the Director chooses and formulates strategic programs.
Conclusion
The panel concludes that the mandate of the INMHA should be maintained. The Institute should pursue an integrative and balanced approach across its fields of research. To facilitate this integrative approach, the panel advises that CIHR and the Institute consider a change to a name that better represents a common focus on the brain. Although too early to assess the impact of the changes resulting from Institutes Modernization in 2014-15 on INMHA, the panel identifies the need for CIHR and the Institute to monitor the potential risk that current resources may not be sufficient to fulfil its mandate.
Recommendation 2: The Panel recommends that the INMHA’s current mandate not change at this time.
Recommendation 3: The Panel recommends that CIHR and INMHA monitor the ability of INMHA to fulfil its mandate with current resource levels.
Recommendation 4: The Panel recommends that CIHR and INMHA should consider changing the name of the Institute to reflect the wider evolution towards ‘brain science.’
Recommendation 5: The Panel recommends that CIHR and INMHA recruit an Institute-specific Advisory Board from the research community to advise and inform the Scientific Director. This INMHA-focused Board could include representatives from the research-focused national associations representing most neuroscience researchers in Canada as a means to ensure that strategic programs are formulated with maximum input from the community.
Observations for the Next Scientific Director and Future Directions
Observations on recruiting the next Scientific Director
As the current Scientific Director of INMHA is at the end of his second term, the panel is not concluding on the question of renewal. The panel has however made some observations to the Governing Council pertaining to the recruitment of the next Scientific Director, should the Institute be retained.
First, the next Scientific Director of INMHA should be a top ranked, well-known scientist to maintain the current credibility and influence of the position, not jeopardize the future of the Institute, and continue the leadership that CIHR currently holds in the areas of neuroscience, mental health and addiction. In addition, a continuing decrease in the Institute’s research budget directly controlled by the Scientific Director could negatively impact the attractiveness of the role and CIHR’s ability to attract excellent candidates.
Next, it will be important for CIHR to provide clarity on key functions and priorities of the next Scientific Director and how they will be evaluated. Broadly, there are three key areas that the Scientific Director can be evaluated on: convening and catalyzing research; working with other Institutes to develop and deliver large research initiatives; and working internationally to raise the profile of, and partnering opportunities for, the Institute and CIHR. While not mutually exclusive, CIHR should give the Scientific Director direction as to where most of their time should be spent and the expected achievements.
Observations on future directions for the Institute
The panel believes that the key challenge facing INMHA and the next Scientific Director will be to mobilize and integrate the research and stakeholder communities behind large initiatives and continue to catalyze international presence and partnerships. INMHA will need to remain vigilant in linking its distinct research communities as well as its partners and stakeholders through working effectively with Brain Canada, Genome Canada, the national associations representing neuroscience researchers (e.g., Canadian Association for Neuroscience (CAN) and the Canadian College of Neuropsychopharmacology (CCNP)) and the health charities as well as their associations (e.g., the Neurological Health Charities Canada (NHCC)).
To be effective at mobilizing and integrating the community, INMHA should be an active player in determining what Canada’s major orientation for brain research should be in the future. By playing a major role in bringing stakeholders together in a national brain initiative, the Scientific Director and Institute will be well placed to enhance Canada’s position in large international initiatives.
Other Observations
In addition to responding to the evaluation questions, there are several other observations that merit the attention of Governing Council.
First, CIHR could consider re-opening the question of whether Institutes should continue to have equal funding or whether Institute funding should be scaled to the burden and economic cost of disease (or to the relative size of research activity in this area). In the case of INMHA, this could involve major investments in mental health research.
Next, it is clear that CIHR wants to ensure that Scientific Director s are acknowledged leaders in their fields. The panel expressed concern that the attractiveness of the Scientific Director position is decreasing given the resources limitations that constrain the ability of the Scientific Director to develop and fund initiatives and engage partners.
Evaluation Overview and Key Findings
Overview
The Canadian Institutes of Health Research (CIHR) has conducted this evaluation of the Institute of Neuroscience, Mental Health and Addictions (INMHA) as part of the suite of rolling evaluations of all CIHR Institutes. The aims of the evaluation are to:
- Provide Governing Council with valid and reliable findings to inform decisions regarding whether the Institute’s role and functioning should be amended, merged, or terminated; and
- Provide CIHR management with valid, insightful, and useful findings regarding the ongoing institute relevance and performance.
The evaluation drew on multiple lines of evidence, including qualitative and quantitative data sources. It collected data from the range of INMHA stakeholders and beneficiaries, including researchers, funding partners, and research users, and integrated these with administrative data on expenditures and publications related to INMHA mandates, using a framework that will be common to all Institute evaluations. While each line of evidence has limitations, there is convergence among them as to key findings. Overall, we are reasonably confident that the results presented here provide an accurate portrait of INMHA’s relevance and performance.
The evaluation was conducted by the CIHR Evaluation Unit and a team of external evaluation professionals and overseen by a panel of experts in INMHA’s mandate areas who reviewed and interpreted the findings and made the final recommendations.
Key Findings
Relevance
Ongoing relevance of support to INMHA research
The evaluation lines of evidence converge to reaffirm that CIHR and Canadian federal investment in neurosciences, mental health, and addictions remains extremely important and relevant. However, over the last decade, INMHA’s external landscape has been shifting, with the addition of new players whose roles and relationships with INMHA are not as yet fully clear to its stakeholders. INMHA’s overall relevance within the CIHR slate is likely also best understood in the context of these external changes and the reasons that underlie them. It seems that there has been a mobilization of private and consumer efforts and funding to accelerate brain-related research; on the whole, this may be an important complement to INMHA’s limited resources and flexibilities. At the same time, the new players’ presence along with significant federal research funding outside INMHA appears to raise a question about INMHA’s future relevance to consumers and other funders including the federal government. In general, these shifts suggest that INMHA’s singularity and prominence may be decreasing.
Appropriateness of Current INMHA mandate
The advisability of retaining INMHA’s broad mandate has been questioned, on two related grounds.
First, the mandate is extremely broad and growing as new fields of research emerge – while at the same time its resources have remained stable or decreased. Within the new CIHR parameters of collective impact through large multi-institute initiatives, INMHA has been a contributor and often a leader, but portions of its community appear to be losing, or at least failing to gain, connectedness to INMHA and CIHR – in particular: its basic neurosciences researcher community; mental health and addictions researchers whose focus lies outside of biomedical sciences; and the health charities with whom some partnerships have languished. Funding from organizations other than CIHR is pervasive and diverse, suggesting that other organizations are also responding to research needs in these mandate areas.
Second, the evaluation data confirm that there is a relative dominance of neuroscience compared to mental health and addictions research, in terms of both investments and impacts. For example, data on INMHA mandate-related expenditures for CIHR as a whole show that while investments have increased since 2001, spending in neurosciences has increased more substantially and more rapidly than in addictions and senses, and that spending in the area of mental health may have decreased overall. These findings suggest, as some in the community do argue, that separating INMHA’s mandate into smaller components would be fruitful, so that addictions and mental health research could be more adequately nurtured. On the other hand, the increased investments in neurosciences may reflect that the neuroscience community is much larger than those other communities, and many neuroscientists define themselves as also being part of the mental health, addiction, and senses communities.
Changes to Institute Name
There is apparent support for the “Brain Research Institute” form of name among influential stakeholders. Proponents of this name argued that the current name is too wordy and yet does not cover all of the domains addressed by the Institute; others suggested that mental health and addictions are essentially assumed under brain science and thus could be dropped from the name. At the same time, the evaluation showed that there is increasing public and political recognition of the urgency to act on the population burden of mental health and addictions. The consequences of removing these areas from the Institute name have not been yet fully considered.
Funding landscape
Research funded by CIHR in the INMHA mandate area constitutes a significant proportion of total CIHR investments. On average, investments in research relating to INMHA’s mandate represented 24% of total CIHR investments over the period from 2000-01 to 2014-15. Total investments in 2014-15 in this area were $229.6M, primarily through investigator-initiated research (e.g. Open Operating Grant Program). (See Figure 2 in Appendix 2). Only the Institute of Genetics and the Institute of Infection and Immunity have a higher proportion of investments in their mandate areas at 34% and 26% respectively.
In 2014-15, CIHR provided funding support to a total of 11,355 health researchers and trainees, of whom 3,624 (32%) were in INMHA mandate areas.
In addition to overall CIHR funding in neuroscience, mental health and addictions, INMHA allocates funding for strategic Institute initiatives. Although fixed in principle at $8.6M annually, this funding amount has changed over time. Recently, this fixed amount witnessed an overall funding decrease. According to the Scientific Director’s presentation to the Institute Evaluation Panel and follow-up with the Scientific Director:
Because of a significant budgetary shortfall, Institutes have been working with minimal discretionary funds. In the current 2016-17 fiscal year, INMHA’s unallocated funds totaled $980K and remains below the full annual baseline allocation of $4.3M until at least the 2023-24 fiscal year.Footnote 8
Overall, these changes signify that while INMHA, like all Institutes, now has more opportunity to pool resources in larger cross-cutting initiatives, it also has had less budgetary room than previously to engage in INMHA-only strategic initiatives. The Institute-managed budget, as prepared by the Institute, is summarized in Figure 3.
In addition, data on INMHA mandate-related expenditures for CIHR as a whole show that while investments have increased since 2001, spending in neurosciences has increased more substantially and more rapidly than in addictions and senses, and that spending in the area of mental health may have decreased overall as illustrated in Figure 4.
CIHR’s budget of $1B for 2015-16 is significantly smaller than the budget of the National Institutes of Health (NIH) budget of $30.3B US dollars for the same year.Footnote 9 While benchmarking comparisons are not easy to establish between the investments made by CIHR in INMHA’s mandate areas and the NIH institutes, a comparison between four NIH institutes with a similar thematic mandate to INMHA shows that CIHR’s mandate investment in INMHA’s mandate areas remains significantly lower than those made by the NIH in the United States.Footnote 10 For example, in 2014 CIHR spent $131.1M in the area of neuroscience whereas the NIH spent $5.6B, which on population basis, represents close to five-fold (4.7) less spending per capita in CanadaFootnote 11 than in the USFootnote 12. This discrepancy/difference in investments made in Canada and the United States must be taken into consideration when reviewing in INMHA’s investments since it has an impact on the amount and quality of research that gets funded in these mandate areas in Canada.
Emergence of New Players in INMHA Ecosystem
In the last ten years, newly funded federal organizations have emerged within INMHA’s research space, with particularly significant investments through the Brain Canada Foundation and Mental Health Commission of Canada (MHCC). In 2011, the Government of Canada announced the establishment of the Canada Brain Research Fund with a $100M commitment to encourage Canadians to increase their support of brain research, and maximize the impact and efficiency of those investments.Footnote 13 The federal government also committed $130M over 10 years in 2007 to establish the MHCC, an arm's length, not-for profit organization designed to improve health and social outcomes for people and their families living with mental illness.Footnote 14
Findings from interviewees suggest that there is some confusion among stakeholders about roles and specificities of new players and CIHR. However, a recent evaluation of the contribution to the Canadian Brain Research Foundation (CBRF) shows that while CBRF may slightly overlap with CIHR offerings, CIHR and Brain Canada are more complementary than duplicative. This complementarity, however, reflects that CBRF funds in areas that CIHR previously had significant programs in such as team grants and infrastructure support, and that CIHR, with relatively flat budgets in the past ten years had de-emphasized. Brain Canada, which administers the CBRF, has a mandate quite different than CIHR, based upon a partnership model to encourage and maximize new funding from the private sector and philanthropy.Footnote 15 CIHR is traditionally the recipient of federal health research funds and collaborates with research institutes, foundations and charities that are diverse in terms of geography, focus and capacity. CIHR pursues research objectives through their 13 different institutes, whereas Brain Canada is as a research organization solely focused on the neurosciences.
The recent evaluation of Health Canada’s contribution to Brain Canada found that the most commonly cited difference between CIHR and CBRF was Brain Canada’s funding of research teams versus individual investigators. CBRF has funded 138 projects in the first few years of its existenceFootnote 16; whereas, CIHR funded 7,247 grants (new and ongoing) in INMHA’s mandate areaFootnote 17 between 2011-12 and 2015-16 (of which 229 were team grants).Footnote 18
The evaluation concludes that INMHA and Brain Canada’s objective are more complementary rather than duplicative and that the CIHR investments in neurosciences, mental health, and addictions remain extremely important and relevant. CIHR remains by far the primary funder, both in terms of investigators funded and projects awarded of neuroscience research in Canada. The lack of a partnership requirement for investigators and institutions for all of CIHR grants and awards is a significant difference between CIHR’s funding model and that of Brain Canada’s recent team grant programs.
Key informant interviews also suggested that INMHA’s partnerships with organizations representing its patient communities, such as the health charities, have changed in the last several years. Research user partners from these organizations indicated that their previous relationship with IMNHA has declined on intensity; for example, co-funded initiatives have not been continued. These research user partners indicated that they are increasingly developing partnerships with other research funding organizations, such as provincial funders, foundations including Brain Canada and the private sector. They are also experiencing increased application pressure, attributed to changes in CIHR funding structure. Altogether, these changes are affecting overall relevance of INMHA in the neurosciences, mental health and addictions research landscape, insofar as the ecosystem of relationships among stakeholders and their relative importance has been shifting. In general, these shifts suggest that INMHA’s singularity and prominence may be decreasing.
Transformative Impact
With respect to the extent to which INMHA has achieved transformative impacts, it is clear that resource pressures from a very large and disparate community have challenged its capacity to satisfy all stakeholders. That being said, it has generally been effective in all of the performance areas assessed.
Support to Innovative Research and Advancing Knowledge
The evaluation found that INMHA is supporting excellent, innovative research that has high impact within its scientific communities. Canada’s stature and influence, as measured by scientific publications and their impact, is above what would be expected in terms of its size in its mandate areas, although more so in neurosciences than addictions or mental health (Figure 5). These findings are not, however, directly attributable to INMHA funding: neuroscience in general is very well-supported in CIHR open competition. In 2014-15, INMHA research spending represented 3.8% of overall CIHR spending in neurosciences, mental health and addictions. For some, this suggested that there is less need for strategic support from the Institutes in neuroscience than in the other areas of its mandate; others argued that it is because of this competitiveness that there is a need for the Institute to capitalize on strength to increase leveraging.
There was consensus among stakeholders that the Institute’s use of its strategic funding has contributed to advancing knowledge, in multiple ways. INMHA funding has filled gaps where open funding was inaccessible to researchers through open competition, and has used funding through inter-institute partnerships to address emerging research areas. The case studies confirmed that research supported by the Institute is positioned to demonstrate innovativeness, excellence, and impact.
The bibliometric analysis strongly confirms that Canadian research in INMHA domains has attained and is maintaining international excellence. Compared to other countries, Canada has strong publication performance in overall health research, ranking 7th or 8th overall depending on the year. In INMHA mandate areas, Canada’s global rank in terms of number of papers published is above its world rank out of the top ten research producing countries studied: 4th in the world in number of addiction research publications, 5th in both mental health and neurosciences, and 6th in research related to the senses. Analysis of INMHA-mandate related publications, citations and co-authorship showed that there has been an increase since the previous assessment in all countries’ research activities (except the US) in all three domains (neurosciences, mental health, and addictions research). This is primarily attributable to an increase in international collaboration.
When research impact is measured as citations, Canada’s rankings in terms of impact, as measured by average of relative citations (ARC), are as follows: addiction (7th), mental health (5th), neurosciences (3rd) and senses (5th). In terms of the top 10% most cited papers, Canada is consistently higher than the proportion of world papers, with neurosciences ranking 5th, mental health and senses (6th) and addictions research (7th). In terms of the specialization index, Canada is the most specialized country in neurosciences, 2nd in senses, and 4th in mental health and addiction. Overall these findings display a relatively high level of research excellence.
Contribution to Building the Capacity of the Health Research Enterprise
The evaluation documented that INMHA’s investment in training has been mainly indirect, relying on grant holders to incorporate research training in their operations, rather than investing in strategic training initiatives, at least in recent years. Expenditure data indicated that INMHA’s funding since 2000 has allocated about 2% of funds provided to scholarships and fellowships; this is less than the proportion (8%) provided to INMHA domains by non-targeted CIHR programs. The expenditure data is corroborated by key informants who noted that INMHA has not recently prioritized capacity building. While INMHA prioritized investment in CIHR’s Strategic Training Initiatives in Health Research (STIHR), this program is no longer active and INMHA-specific training may be eroding.
As the strategic lead on the Canada-China Joint Health Research Initiative (CCJHRI), INMHA worked closely with other CIHR Institutes to establish a strong working relationship National Natural Science Foundation of China (NSFC). First established in 2006, CCJHRI resulted in the ‘twinning’ of 135 Canadian labs with 135 Chinese partners. The initiative was formally evaluated and found to be mutually beneficial to both Canadian and Chinese researchers paving the way for a third phase of this partnership.
Contribution to achieving broader health, economic and social impacts
INMHA is making some contributions to CIHR’s overall directions and priorities in terms of advancing impacts on health services and population health, within the opportunities afforded by the state of science in its mandate domains – said to be often far from clinically-relevant knowledge transfer. Evaluation findings showed that when INMHA has had the resources and opportunities to support research that can be closely and immediately linked to health systems and population health improvements, it has had considerable success fostering the necessary linkages and infrastructure to ensure impact. Overall, however, multiple sources of evaluation data indicated that INMHA’s contribution to date to improved health systems and population health has not been strong. As well, INMHA’s research community is not strongly aligned with CIHR strategic priorities. The survey data indicated that a significant group of researchers does not identify with CIHRs current priorities: 93 researchers (26%) indicated that none of the CIHR five strategic investment priorities fit with their research.
The evaluation did nonetheless find suggestive evidence that INMHA-mandate research (although not necessarily INMHA-funded) has influenced a wide range of policies and practice guidelines that have the potential for important impacts on population health. The study of INMHA publication impact outside of academia found some policies influenced by the 3% of 2008-2009 publications could have implications for large populations: e.g., Hockey Canada's Board of Directors voting to eliminate body checking for peewee players at its Annual General Meeting in 2013.Footnote 19
Evidence indicates that commercialization of research results is not an area of strength for this Institute, with funding supporting commercialization to limited extent given its ongoing focus on basic science and lack of interest from the private sector. Indeed, 8% of surveyed researchers (who indicated it applied to them) reported that their INMHA funding supported commercialization of research findings; whereas, one-third (31%) indicated commercialization did not apply to them. Nevertheless, six percent of survey respondents reported that it had helped share findings with private sector firms, and about 5% of INMHA publications in 2008-09 had influence in creating a total of 102 patents by 2015.Footnote 20
Convener and Catalyst
Partnering to achieve CHIR and Institute Objectives
The evaluation found that INMHA has been an effective convener and catalyst. In INMHA mandate domains, Canadian research’s stature and prospects have been enlarged by significant strategic partnerships and co-funding with other Institutes and Canadian and international organizations. Significant examples are available of initiatives that have allowed Canadian researchers access to resources that would not otherwise have had and that are positioned to accelerate discovery over and above what would have happened in the absence of INMHA efforts.
The Institute and its leadership have been highly proactive in identifying, seizing, and creating opportunities to advance INMHA-domain research through strategic partnerships. INMHA leadership has excelled in establishing collaborations with important international research entities, including: the China-Canada Collaboration depression research, the International Human Epigenome Consortium, which INMHA has expanded to include a partnership with the Japan Science and Technology Agency. Again, due to the limited institute strategic budget and a requirement to develop most initiatives with other Institutes, there is only a limited ability to impact the research of the vast majority of the community represented by INMHA.
Increase in Partners contributions
A key success of the Institute has been the creation and fostering of partnerships with researchers, knowledge users and funders. INMHA’s partnerships have resulted in increased leveraging of additional funding from $7.9M for the period from 2001-02 to 2007-08 to $31.9M for the 2008-09 to 2014-15 period. Notably among international partner contributions to INMHA funded research increased sharply from $1M to $17.5M (17-fold increase), not-for-profit partner contributions increased from 730K to $8.3M, and for-profit partner contributions increased from $1.2M to $1.8M over the two periods (Figure 1 in appendix 2).
This is consistent with the re-orientation announced in its Strategic Plan 2012 -2017 of a heightened strategic focus on playing a connector role and on seeking opportunities through partnerships to influence the entire continuum of care.
International contributions accounted for 47% of the total partner contributions, the Not-for-Profit sector accounted for 23% and the for profit sector contributions accounted for 8%. Table 1 provides a list of the top investors in INMHA mandate.
At the same time, the evaluation found that some former and potential partners find themselves working with alternative research funding partners to INMHA, as its attention and interest in them appears to have waned over time. This may be having negative consequences in terms of donor mobilizability for INMHA-relevant research.
Visibility and Profile
Over and above the profile created by successful partnerships within Canada and internationally, INMHA has engaged in a number of activities to increase its visibility and profile among researchers, knowledge users, stakeholders and the public.
The case study of INMHA’s response to traumatic brain injury (TBI) completed as part of this evaluation provides an example of the leadership of the Scientific Director and Institute to seize a fortuitous opportunity to join ranks with and contribute to key international initiative called the International Initiative for Traumatic Brain Injury Research (InTBIR). In bringing Canada to this table, INMHA opened a window for the existing highly developed Canadian research capacity in TBI. INMHA played a key role by convening a national workshop, in partnership with the Ontario Neurotrauma Foundation (ONF), to advance the Canadian TBI research agenda and, subsequently, co-funding a four-year team grant called the Canadian Traumatic Brain Injury Research Consortium (TBIRC); funding partners are INMHA ($1.6M), Institute of Aging ($125,000), Institute of Genetics ($62,500) and the ONF ($175,000). The team grant is seen as highly effective in creating a new cohesion among Canadian researchers and giving them access to networks and resources that they were not able to use before, both within and outside of Canada. CIHR, however, as a founding partner for this and other strategic initiatives, should ensure that they continue to operate on a model whereby all Canadian researchers have access to and should be able to apply for funding in open competitions.
Researchers involved in TBIRC reported that this membership alone has increased their productivity because they have committed to producing results for and with international partners.
Contribution of Scientific leadership to convener-catalyst role
It is clear from key informant interviews that the INMHA scientific leadership is highly regarded. Over and above strong reputations as scientists, the INMHA leadership team was cited as particularly gifted in anticipating movement and its momentum in their research fields, and highly skilled and energetic at facilitating conversations and building platforms to advance opportunities for knowledge development and translation.
Although external stakeholders cited INMHA scientific leadership as exemplary among Institutes, there were mixed views on the leadership’s role within and contribution to the transformative objectives of CIHR.
Operational Effectiveness
INMHA Effectiveness
Evidence indicates that INMHA, as an entity, has been highly successful over the last decade, benefitting from strong leadership and adequate support from its host institution and CIHR. The Institute has effectively implemented its strategic and operational plans, through launch of approximately 140 Requests for Applications and Priority Announcements. For the period from 2009-10 to 2015-16, INMHA’s Institute Support Grants (ISG) expenditures of $6.4M to establish and sustain Institute operations, events, and activities were allocated as follows: about one-third (36%) to community engagement and two-thirds (64%) to operating the Institute. It is seen as a highly effective organization given its limited resources; however, questions were raised as to whether sufficient resources were in place to be able to achieve the Institute’s strategic goals.
Support provided by CIHR
Views exist both within and outside CIHR that the change in IAB structure has significantly reduced all institutes, including INMHA’s, connection to its user communities.Footnote 21 While there is understanding of the overall need for reforms, some interviewees, both internally and externally believe that the new structures signal CIHR’s intent to lower the prominence or perhaps even dismantle the Institutes in general. In this context, it is not surprising that findings on the effectiveness of the INMHA – CIHR-central interface are variable, with both strength and concerns identified.
References
Dybdal, L., Nielsen, S. B., Lemire, S. (2011). Contribution Analysis Applied: Reflections on Scope and Methodology, Canadian Journal of Program Evaluation, 25(2), pp. 29-57.
Jabalpurwala, I. (2016). Brain Canada Foundation. Neuron. No.2: vol. 92 (3) pp-601-606.
Lancet Neurology (2012). The Changing Landscape of Traumatic Brain Injury. Science Spical Issue, the Aging Brain.
Marchildon, G. P. (2013). Canada: Health System Review. Health Systems in Transition. Vol. 15. No. 1. University of Regina. Canada.
Mayne, J. (2001). Addressing Attribution Through Contribution Analysis: Using Performance Measures Sensibly, Canadian Journal of Program Evaluation, 16 (1), pp.1-24.
Mayne, J. (2011). Contribution Analysis: Addressing Cause and Effect, in Kim Forss, Mita Marra and Robert Schwartz, Evaluating the Complex: Attribution, Contribution, and Beyond, New Brunswick, Transaction Publishers, pp.53-95.
Mayne, J. (2012). Making Causal Claims, CES Ottawa, October 2012.
Mayne, J. (2015). Useful Theory of Change Models, Canadian Journal of Program Evaluation, 30(2), pp.119-142.
Mental Health Commission of Canada. Changing directions, changing lives: The Mental Health Strategy for Canada [ PDF (11.7 MB) - external link ], (2012).
Ostry, A. (2006). Change and continuity in Canada’s health care system. Ottawa, CHA Press.
Performance and Accountability Branch (PAB) , CIHR Institute of Neurosciences, Mental Health and Addiction (INMHA): Mandate-Related Knowledge Production and Impact Report (2008-2015), October 20, 2016, Table 3, p. 5.
Pollitt, A., Cochrane, G., Kirtley, A., Krapels, J., Larivière, V., Lichten, C., Parks, S., and Wooding, S. (2016). Mapping the Global Mental Health Research Funding System. Rand Europe. Cambridge, UK.
Skinner, W. J., O’Grady, C., Bartah, C. and Parker, C. (2011).Concurrent Substance Use and Mental Health Disorders: An Information guide.
Larivière,V. and Macaluso, B. (2016). Observatoire des sciences et des technologies, Centre interuniversitaire de recherche sur la science et la technologie, Bibliometric Analysis of INMHA-Related Research, 2000-2015.
World Health Organization (WHO). Comprehensive Mental Health Action Plan: 2013-2010.
World Health Organization (WHO). Dementia: a public health priority.
Yuste, R. and Church, G. (2014). The New Century of the Brain, Scientific American, 310, pp. 38-45.
Appendix 1: Overview Data Sources and Methods
| Data source | Description | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Situational analysisFootnote 22 |
|
||||||||||||||||||
| Bibliometric analysisFootnote 23 |
|
||||||||||||||||||
| Key informant interviews |
|
||||||||||||||||||
| Researcher survey |
|
||||||||||||||||||
| Case studies |
|
||||||||||||||||||
| Study of INMHA publication impact outside of academiaFootnote 25 |
|
These data sources were complemented by telephone consultations carried out by the Institute Evaluation Panel during its two-day face-to-face meeting, with six key members of the INMHA research community who had not been previously interviewed (although some had competed the researcher survey).
Appendix 2: Figures and Tables
Figure 1: Partner Contributions to INMHA funded research 2000-07- 2008-14
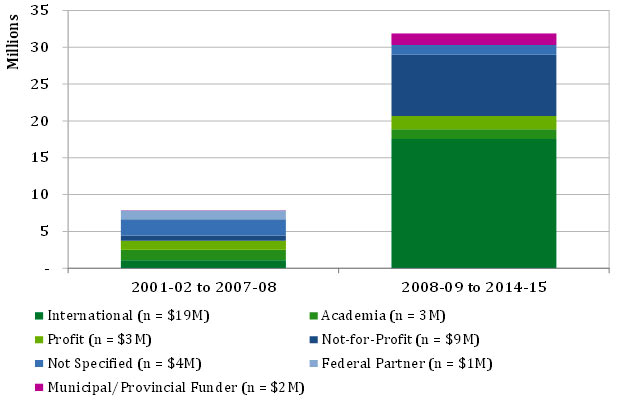
Figure 1 – long description
| 2001-02 to 2007-08 | 2008-09 to 2014-15 | Total | |
|---|---|---|---|
| Federal Partner (n = $1M) | 1,175,000 | - | 1,175,000 |
| Municipal/Provincial Funder (n = $2M) | 46,250 | 1,578,560 | 1,624,810 |
| International (n = $19M) | 1,083,376 | 17,541,409 | 18,624,785 |
| Academia (n = 3M) | 1,403,566 | 1,323,172 | 2,726,738 |
| Profit (n = $3M) | 1,234,677 | 1,808,772 | 3,043,449 |
| Not-for-Profit (n = $9M) | 730,866 | 8,331,606 | 9,062,472 |
| Not Specified (n = $4M) | 2,200,274 | 1,323,172 | 3,523,446 |
| Total | 7,874,009 | 31,906,691 | 39,780,700 |
Figure 2: CIHR Investment in INMHA mandate area, by type, 2000-2014
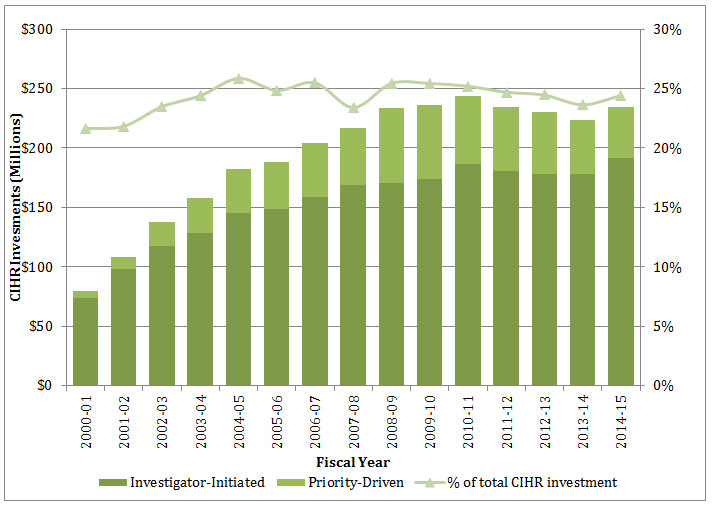
Figure 2 – long description
| total | 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Investigator-Initiated | 2,299,547,304 | 73,862,430 | 98,243,615 | 117,851,115 | 128,127,893 | 145,310,224 | 148,670,748 | 158,480,435 | 168,526,511 | 170,585,214 | 174,112,786 | 186,924,174 | 180,996,534 | 177,942,071 | 178,292,009 | 191,621,547 |
| Priority-Driven | 611,849,907 | 6,195,693 | 9,733,006 | 19,990,594 | 29,718,317 | 36,957,811 | 39,773,821 | 45,420,137 | 48,472,742 | 62,691,654 | 62,245,531 | 56,806,306 | 53,844,057 | 52,198,870 | 44,899,525 | 42,901,843 |
| Grand Total | 2,911,397,211 | 80,058,123 | 107,976,620 | 137,841,709 | 157,846,210 | 182,268,035 | 188,444,569 | 203,900,571 | 216,999,253 | 233,276,868 | 236,358,318 | 243,730,479 | 234,840,591 | 230,140,941 | 223,191,534 | 234,523,390 |
| CIHR investments overall | 11,895,401,578 | 369,833,297 | 494,540,211 | 586,826,186 | 646,850,893 | 704,689,215 | 758,146,346 | 799,646,533 | 926,716,411 | 916,875,687 | 929,144,803 | 966,828,661 | 950,729,984 | 940,773,074 | 943,955,267 | 959,845,009 |
| % of total CIHR investment | 24% | 22% | 22% | 23% | 24% | 26% | 25% | 25% | 23% | 25% | 25% | 25% | 25% | 24% | 24% | 24% |
Figure 3: INMHA Institute Strategic Budget, 2009-2015.
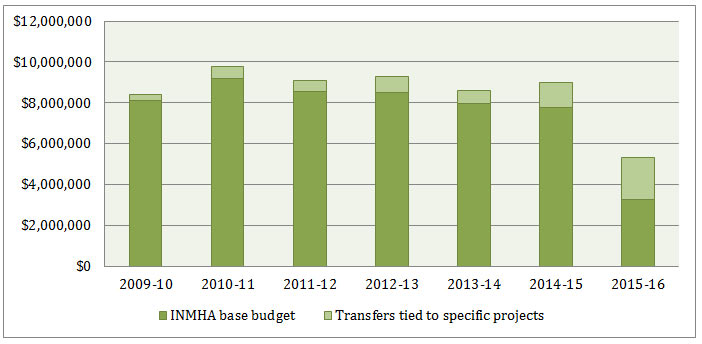
Figure 3 – long description
| 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | |
|---|---|---|---|---|---|---|---|
| INMHA Base Budget | $7,883,107 | $9,193,441 | $8,530,596 | $8,500,955 | $7,958,245 | $7,754,749 | $3,263,782 |
| Transfers tied to specific projects | $310,000 | $600,000 | $585,750 | $766,857 | $630,927 | $1,230,250 | $2,035,000 |
Figure 4: CIHR spending in INMHA mandate areas, 2000-2014
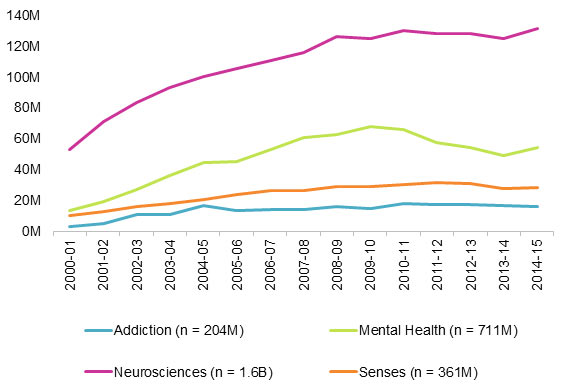
Figure 4 – long description
| total | 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Addiction (n = 204M) | 204,765,591 | 2,934,098 | 4,895,979 | 11,126,816 | 10,892,474 | 16,992,847 | 13,545,211 | 14,003,424 | 14,083,916 | 15,865,194 | 14,566,702 | 18,098,246 | 17,242,471 | 17,384,088 | 16,869,346 | 16,264,778 |
| Mental Health (n = 711M) | 710,783,327 | 13,570,509 | 19,212,466 | 27,231,764 | 35,889,593 | 44,595,497 | 45,507,026 | 53,046,217 | 60,426,205 | 62,755,195 | 67,699,314 | 65,715,161 | 57,640,532 | 54,139,502 | 49,361,980 | 53,992,366 |
| Neurosciences (n = 1.6B) | 1,625,430,702 | 53,038,913 | 70,835,568 | 83,603,242 | 93,186,638 | 100,273,185 | 105,585,666 | 110,691,656 | 115,840,187 | 125,867,172 | 124,822,645 | 129,652,053 | 127,991,508 | 127,950,387 | 124,946,208 | 131,145,675 |
| Senses (n = 361M) | 360,861,166 | 10,514,603 | 13,032,606 | 15,879,886 | 17,951,031 | 20,470,757 | 23,870,916 | 26,254,066 | 26,712,696 | 28,805,244 | 29,184,279 | 30,094,265 | 31,544,222 | 30,785,842 | 27,575,231 | 28,185,521 |
Source: INMHA Situational analysis, data from CIHR EIS.
Figure 5: Proportion of world papers and of top 10% most cited papers, Canada, 2000-2014
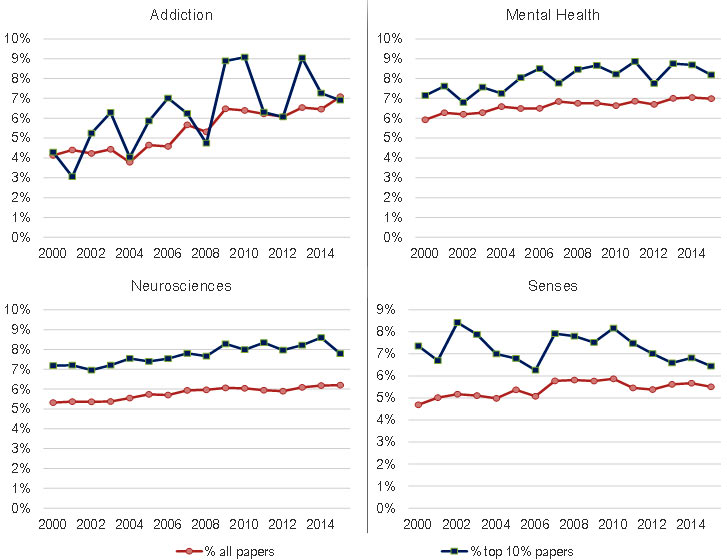
Figure 5 – long description
| Addiction | Mental Health | Neurosciences | Sciences | |||||
|---|---|---|---|---|---|---|---|---|
| % all papers | % top 10% papers | % all papers | % top 10% papers | % all papers | % top 10% papers | % all papers | % top 10% papers | |
| 2000 | 4% | 4% | 6% | 7% | 5% | 7% | 5% | 7% |
| 2001 | 4% | 3% | 6% | 8% | 5% | 7% | 5% | 7% |
| 2002 | 4% | 5% | 6% | 7% | 5% | 7% | 5% | 8% |
| 2003 | 4% | 6% | 6% | 8% | 5% | 7% | 5% | 8% |
| 2004 | 4% | 4% | 7% | 7% | 6% | 8% | 5% | 7% |
| 2005 | 5% | 6% | 6% | 8% | 6% | 7% | 5% | 7% |
| 2006 | 5% | 7% | 6% | 9% | 6% | 8% | 5% | 6% |
| 2007 | 6% | 6% | 7% | 8% | 6% | 8% | 6% | 8% |
| 2008 | 5% | 5% | 7% | 8% | 6% | 8% | 6% | 8% |
| 2009 | 6% | 9% | 7% | 9% | 6% | 8% | 6% | 8% |
| 2010 | 6% | 9% | 7% | 8% | 6% | 8% | 6% | 8% |
| 2011 | 6% | 6% | 7% | 9% | 6% | 8% | 5% | 7% |
| 2012 | 6% | 6% | 7% | 8% | 6% | 8% | 5% | 7% |
| 2013 | 7% | 9% | 7% | 9% | 6% | 8% | 6% | 7% |
| 2014 | 6% | 7% | 7% | 9% | 6% | 9% | 6% | 7% |
| 2015 | 7% | 7% | 7% | 8% | 6% | 8% | 6% | 6% |
Source: Vincent Larivière, Benoit Macaluso. Observatoire des sciences et des technologies, Centre interuniversitaire de recherche sur la science et la technologie, Bibliometric Analysis of INMHA-Related Research, 2000-2015.
Figure 6: Canada in comparison to other Countries Specialized Index (SI) and Average Relative Citations (ARC)
Addiction
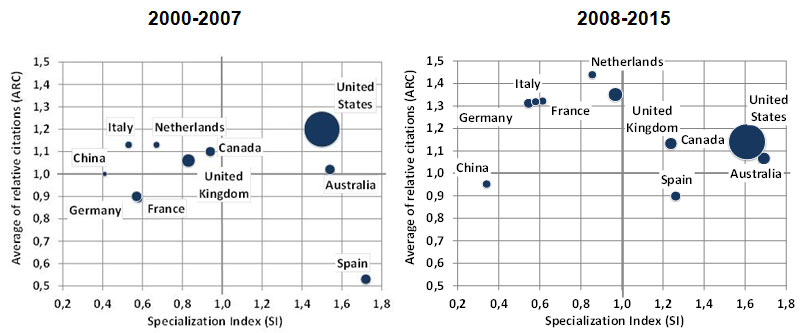
Figure 6 – Addiction – long description
| 2000-2007 | 2008-2015 | |||||
|---|---|---|---|---|---|---|
| Country | SI | ARC | Papers | SI | ARC | Papers |
| Australia | 1.54 | 1.02 | 2031 | 1.69 | 1.07 | 4328 |
| Canada | 0.94 | 1.10 | 1942 | 1.24 | 1.13 | 4035 |
| China | 0.41 | 1.00 | 493 | 0.34 | 0.95 | 1966 |
| France | 0.58 | 0.89 | 1365 | 0.61 | 1.32 | 1856 |
| Germany | 0.57 | 0.90 | 2053 | 0.55 | 1.31 | 2645 |
| Italy | 0.53 | 1.13 | 1037 | 0.58 | 1.32 | 1789 |
| Netherlands | 0.67 | 1.13 | 892 | 0.86 | 1.44 | 1897 |
| Spain | 1.72 | 0.53 | 2058 | 1.26 | 0.90 | 2730 |
| United Kingdom | 0.83 | 1.06 | 3435 | 0.97 | 1.35 | 5417 |
| United States | 1.50 | 1.20 | 24513 | 1.61 | 1.14 | 34917 |
Mental health
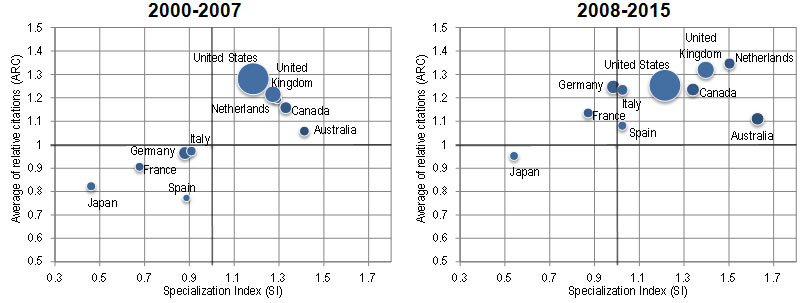
Figure 6 – Mental health – long description
| 2000-2007 | 2008-2015 | |||||
|---|---|---|---|---|---|---|
| Country | SI | ARC | Papers | SI | ARC | Papers |
| Australia | 1.41 | 1.06 | 6926 | 1.63 | 1.11 | 17190 |
| Canada | 1.33 | 1.16 | 10193 | 1.34 | 1.24 | 18009 |
| France | 0.68 | 0.91 | 5931 | 0.87 | 1.14 | 10885 |
| Germany | 0.88 | 0.97 | 11779 | 0.98 | 1.25 | 19670 |
| Italy | 0.91 | 0.97 | 6608 | 1.02 | 1.23 | 13054 |
| Japan | 0.46 | 0.82 | 6047 | 0.54 | 0.95 | 8543 |
| Netherlands | 1.29 | 1.19 | 6381 | 1.50 | 1.35 | 13750 |
| Spain | 0.89 | 0.77 | 3936 | 1.02 | 1.08 | 9144 |
| United Kingdom | 1.27 | 1.22 | 19615 | 1.40 | 1.32 | 32227 |
| United States | 1.18 | 1.28 | 71924 | 1.21 | 1.25 | 108739 |
Neurosciences
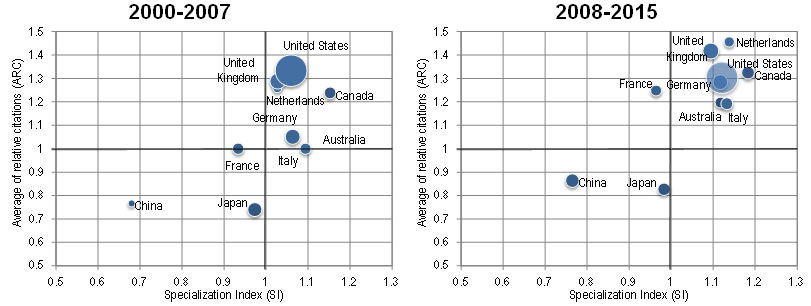
Figure 6 – Neurosciences – long description
| 2000-2007 | 2008-2015 | |||||
|---|---|---|---|---|---|---|
| Country | SI | ARC | Papers | SI | ARC | Papers |
| Australia | 1.06 | 1.07 | 21921 | 1.12 | 1.20 | 43079 |
| Canada | 1.15 | 1.24 | 37140 | 1.18 | 1.32 | 58092 |
| China | 0.68 | 0.77 | 12715 | 0.76 | 0.86 | 66439 |
| France | 0.93 | 1.00 | 34402 | 0.96 | 1.25 | 43974 |
| Germany | 1.06 | 1.05 | 59861 | 1.12 | 1.28 | 81608 |
| Italy | 1.09 | 1.00 | 33456 | 1.13 | 1.19 | 52681 |
| Japan | 0.97 | 0.74 | 53687 | 0.98 | 0.83 | 56743 |
| Netherlands | 1.03 | 1.26 | 21347 | 1.14 | 1.46 | 38037 |
| United Kingdom | 1.03 | 1.29 | 66592 | 1.09 | 1.42 | 92248 |
| United States | 1.06 | 1.33 | 270551 | 1.12 | 1.30 | 366635 |
Senses
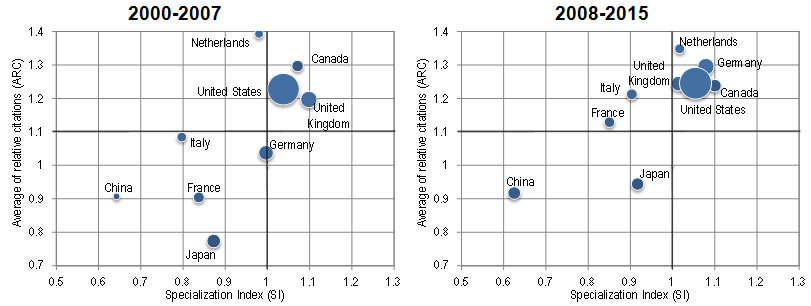
Figure 6 – Senses – long description
| 2000-2007 | 2008-2015 | |||||
|---|---|---|---|---|---|---|
| Country | SI | ARC | Papers | SI | ARC | Papers |
| Australia | 1.32 | 1.19 | 5414 | 1.33 | 1.23 | 10080 |
| Canada | 1.07 | 1.30 | 6870 | 1.10 | 1.24 | 10586 |
| China | 0.64 | 0.91 | 2390 | 0.63 | 0.92 | 10639 |
| France | 0.84 | 0.90 | 6139 | 0.85 | 1.13 | 7600 |
| Germany | 1.00 | 1.04 | 11161 | 1.01 | 1.24 | 14521 |
| Italy | 0.80 | 1.08 | 4850 | 0.90 | 1.21 | 8234 |
| Japan | 0.87 | 0.77 | 9581 | 0.92 | 0.94 | 10367 |
| Netherlands | 0.98 | 1.39 | 4053 | 1.02 | 1.35 | 6659 |
| United Kingdom | 1.10 | 1.20 | 14151 | 1.08 | 1.30 | 17823 |
| United States | 1.04 | 1.23 | 52713 | 1.05 | 1.25 | 67555 |
Source: Vincent Larivière, Benoit Macaluso. Observatoire des sciences et des technologies, Centre interuniversitaire de recherche sur la science et la technologie, Bibliometric Analysis of INMHA-Related Research, 2000-2015.
Table 1: Top 10 investors in INMHA’s mandate
| Top 10 investors in INMHA mandate | Type of invester | # of Grants and Awards | Amount |
|---|---|---|---|
| Astra Zeneca Canada | Profit | n = 103 (44%) | $5,220,373 |
| Canada's Research Based Pharmaceutical Co. | Academic | n = 46 (39%) | $5,727,095 |
| Heart & Stroke Foundation of Canada | Not-for Profit | n = 39 (10%) | $3,395,457 |
| Pharmaceutical Manufacturers Association of Canada | Not-for Profit | n = 20 (6%) | $3,044,611 |
| ALS Society of Canada | Not for profit | n = 16 (4%) | $2,553,850 |
| Neuromuscular Research Program (ALS Society) | Not for profit | n = 13 (3%) | $5,105,516 |
| French National Research Agency | International | n = 12 (9%) | $3,298,175 |
| Federal Ministry of Education and Research | International | n = 11 (8%) | $2,690,774 |
| Academy of Finland | International | n = 8 (6%) | $5,936,528 |
| National Natural Science Foundation of China | International | n = 32 (24%) | $3,828,277 |
Table 2: INMHA strategic investment priorities, as abstracted from 2001-06, 2007-11 and 2012-17 Strategic Plans.
| Strategic Plan 1: 2001-2006 | Strategic Plan 2: 2007-2011 | Strategic Plan 3: 2012-2017 |
|---|---|---|
|
|
|
- Date modified: