Internal Assessment for 2011 International Review - CIHR Institute of Musculoskeletal Health and Arthritis
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Outputs and Outcomes
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures and Tables
- Figure 1: IMHA's focus areas, priorities and KT goals
- Figure 2: Total CIHR expenditures in IMHA's three strategic priority areas
- Figure 3: The IMHA Pipeline
- Figure 4: Percentage of total CIHR expenditures invested annually in IMHA-relevant grants, training and salary awards
- Figure 5: Percentage of CIHR expenditures invested annually in IMHA's focus areas
- Figure 6: Number of peer-reviewed publications obtained or expected from IMHA strategic-initiative research grants by focus area
- Figure 7: Percentage growth (relative to 1997) in contributions to total yearly Canadian papers in IMHA-related areas by CIHR and IMHA strategic initiative-funded PIs
- Figure 8: Number of graduate students trained on strategic initiative-funded research grants
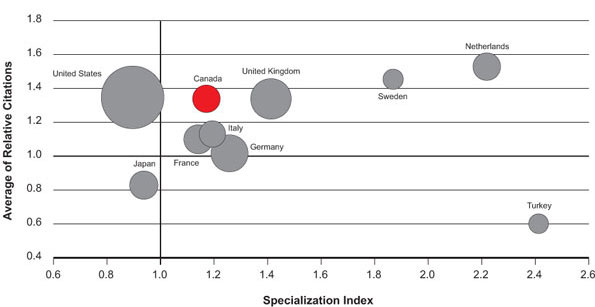
- Figure 9: Specialization index and average of relative citations for top 10 countries
publishing in arthritis, 2000–2008
- Table 1: Leveraging of IMHA funding by partner contributions
- Table 2: Average of relative citation (ARC) values between 2003–2008 of IMHA-related research articles in the top six producing countries, and ARC values for publications of PIs funded by CIHR
Mandate and Context
Mandate, mission and communities
The CIHR Institute of Musculoskeletal Health and Arthritis (IMHA) supports research to enhance active living, mobility and movement and oral health. More specifically, it supports research that addresses causes, prevention, screening, diagnosis, treatment, support needs and palliation for a wide range of diseases and conditions related to the Institute's six foci: arthritis, bone, skin, muscle, musculoskeletal (MSK) rehabilitation, and oral health (Figure 1). The mission of IMHA is to enable the creation and translation of knowledge to improve MSK, skin and oral health. IMHA is unique among Canadian and international funding agencies in its mandate to support research and knowledge translation (KT) across these six discrete foci.
Figure 1: IMHA's focus areas, priorities and KT goals
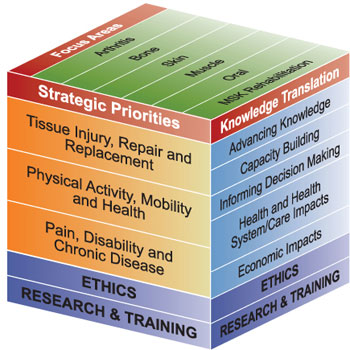
IMHA's six mandated foci are all linked to chronic disease. MSK disorders are the most frequent type of chronic health condition, the most frequent cause of long-term disability, and the most costly health conditions to Canadian society.Footnote 1,Footnote 2 When oral and skin are added, the overall Canadian and global socio-economic burden of chronic diseases and conditions under IMHA's mandate is enormous.
Significant challenges to addressing the chronic disease burden within IMHA's mandate include the breadth of the conditions, the diversity of the research communities (IMHA research spans more than 15 basic and clinical disciplines) and the low capacity and diversity of research strengths within these communities. Despite obvious inter-relationships among components of the MSK system and connective tissues generally in health and disease, at the inception of CIHR, researchers and most of the associated stakeholder communities in IMHA's six foci worked in isolation, in silos with clinical and disciplinary boundaries. Exacerbating the diversity of communities were the differences in size of each community, the arthritis and bone communities being much larger than the skin and oral health communities. With an iterative and inclusive strategic planning process, IMHA succeeded in bringing these communities together around three cross-cutting strategic priorities: Tissue Injury, Repair and Replacement; Pain, Disability and Chronic Disease; and Physical Activity, Mobility and Health (Figure 1). As we document later, these and associated IMHA activities have engendered new cross-focus multidisciplinary research and KT collaborations to tackle previously intractable questions within IMHA's mandate.
In 2009–2010, CIHR invested $74.6 million in grants and awards on research across IMHA-relevant areas, up from $22 million in 2000–2001. CIHR is by far the largest and one of the few funders of MSK, oral and skin peer-reviewed research in Canada. Since its inception, IMHA has built strategies and reversed the low capacity for research and KT across all its foci. It has also focused attention on important burdens of illness in its smaller research communities. This positioned IMHA and its communities to advance on all of its strategic research priorities and tackle the enormous burden of chronic disease within IMHA's mandate.
IMHA is by far the largest funder of MSK, oral and skin health and arthritis research in Canada. IMHA is unique among Canadian and international funding agencies in its mandate to support research and KT across six discrete foci, and has taken a leadership position in convening, unifying and building to meet its mandate.
Institute Priorities
IMHA priority-setting and strategic planning: broad consultation and evidence-informed decision making
The major diseases and conditions under IMHA's mandate and spanning its six foci (Figure 1) are chronic, painful and frequently poorly diagnosed or diagnosed late in disease progression when tissue damage is extensive and reparative processes or therapeutics are limited.Footnote 1,Footnote 2,Footnote 4,Footnote 5,Footnote 6,Footnote 7 The research communities addressing these diseases and conditions are of markedly different sizes and, at the inception of IMHA, were often functionally separate. IMHA championed and continues to use multiple mechanisms to ensure that all voices are heard, including the following:
-
All six foci are represented on IMHA's Institute Advisory Board (IAB), four IAB committees and focus and strategic research priority working groups. Researchers, members of partner organizations, patients/consumers, and external, non-IAB members populate committees and working groups to ensure a breadth of views and to enhance transparency.
-
Broad consultations and workshops have taken place in all foci. One tool unique to IMHA is IMHA on the Move, a large, multi-stakeholder meeting in the format of an open dialogue. The first was held in 2003 to disseminate IMHA's first strategic plan. In November 2006, IMHA hosted IMHA On the Move II, bringing together 34 Canada Research Chairs within IMHA's mandate, other IMHA-related researchers and multiple partner organizations. The conference included the incoming scientific director and stakeholders provided input during breakout sessions and an open forum to help shape IMHA's priorities for its second strategic plan. To gauge progress towards meeting the goals of the second strategic plan and consult on activities beyond 2013, IMHA On the Move III is scheduled for 2011.
-
The Institute has developed an integrated KT model of consensus conferences that includes multiple focus areas, diverse partners representing different sectors, policy makers and other government representatives, and patients/consumers.
-
IMHA participates in annual research conferences in all six of its foci.
Through these and other activities, IMHA has succeeded in bringing together its communities to explore multidisciplinary solutions to health challenges within its mandate. In IMHA's first strategic plan, 2002–2005, the Institute's six foci were spanned by four strategic priorities: Injury, Immunity, Inflammation, Repair and Tissue Engineering; Pain, Disability and Rehabilitation; Mobility, Fitness and Exercise; and Biomaterials and Devices. Throughout late 2006 and 2007, extensive consultations were held to evaluate and reenergize IMHA's priorities, which evolved and coalesced into the three priorities outlined in IMHA's second strategic plan, 2008–2013: Tissue Injury, Repair and Replacement; Pain, Disability and Chronic Disease; and Physical Activity, Mobility and Health (Figure 1).
These high-level research priorities are formulated to encourage recognition of common issues and concerns. For example, Pain, Disability and Chronic Disease incorporates the pain in oral disease and disability, i.e., permanent tooth loss, the pain and disability of osteoarthritis and its rehabilitation implications, and the chronicity of various skin and bone diseases, such as psoriasis and osteoporosis.
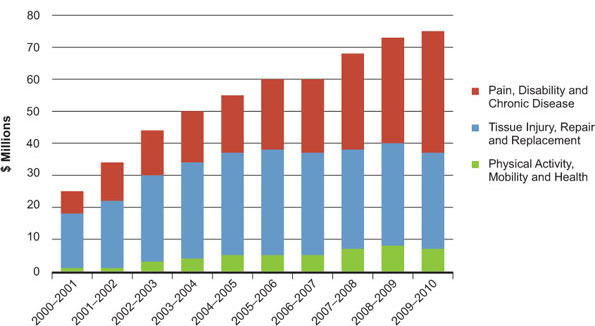
Research activity in each priority area has grown since the inception of IMHA but remains unequal (Figure 2), in part reflecting differing capacities within the areas. The data in Figure 2 reflect, in part, IMHA's annual analysis of grants and awards funded by CIHR using a large set of IMHA-relevant keywords. The entire dataset was revalidated in 2008–2009 to ensure consistency across all years and that a methods approach was standardized for future years. This systematic mining of data from open and strategic competitions in each of IMHA's strategic priorities over time is enabling a comprehensive analysis of strengths, weaknesses, opportunities and threats (SWOT).
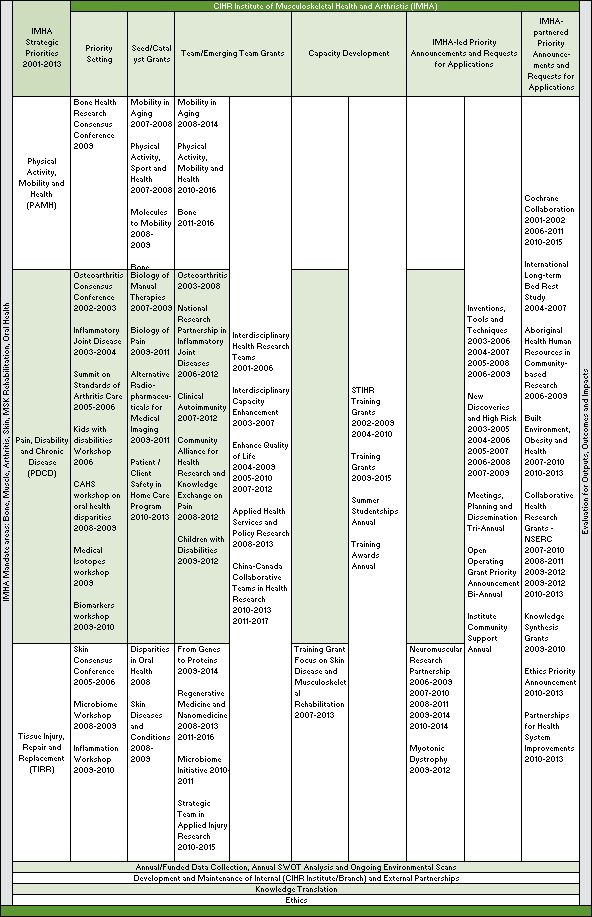
The SWOT data deck is reviewed annually by IMHA's priority working groups and used to inform IAB planning discussions. This has allowed IMHA and its IAB members to make informed and evidence-based strategic decisions, such as those described below under Physical Activity, Mobility and Health (PAMH). In 2009–2010, we expanded our SWOT process by including data acquired by our own in-house, web-based Micro Impact Survey (MIS) tool (described in the Outputs and Outcomes section), which will be very useful for future planning and informing strategic directions. The IMHA pipeline shown in Figure 3 describes the evolution of activities from initial consultations to workshops through to funding opportunities (requests for applications, or RFAs) to build capacity, support multidisciplinary research and address IMHA's strategic priorities.
Figure 2: Total CIHR expenditures in IMHA's three strategic priority areas
IMHA is on a course of continued evolution to maximize its outputs and impacts. The Institute's 2008–2013 strategic plan intensifies its focus on gaps and opportunities related to health systems, and the need for more clinician-scientists to engage in IMHA-related research. The plan highlights that, to maximize the impact of IMHA's strategic initiatives and research funding, the Institute must prioritize and partner strategically and focus its time and efforts on fewer key items with greater investments.
The SWOT data deck documents continued low activity in PAMH even as the burden of chronic diseases (including those under IMHA's mandate) continued to grow.Footnote 1,Footnote 2,Footnote 4,Footnote 5,Footnote 6,Footnote 7 As a result, IMHA recognized the importance of increasing research and KT in the prevention of chronic diseases. IMHA identified PAMH as its flagship priority, and has made a commitment to increase research support and build capacity in this area. To this end, IMHA made its largest-ever commitment to a single program ($6.63 million). With partners bringing the total to almost $10 million, funding for four multidisciplinary PAMH teams was announced by the federal Minister of Health in July 2010. PAMH team research goals are directed towards reducing the burden of chronic diseases by preventing or ameliorating the consequences of juvenile and adult arthritis, cancer and cardiovascular disease. IMHA could not have done this without the cross-focus community building, capacity building and multidisciplinarity it has fostered over time.
Figure 3 highlights the evolution of IMHA's activities and initiatives related to our six focus areas and across our three strategic priorities.
International Review of 2006
The CIHR International Review Panel impression of IMHA was "very good" and its performance was considered high. Key strengths were in the broadening of the discipline base of skin, oral and MSK rehabilitation research and KT, and integrating research across the four themes of biomedical, clinical, health services and policy research, and population and public health. The panel's suggestions included further expanding KT, partnerships, training and the ethics program.
Expanding knowledge translation
IMHA was ahead of the curve in KT in many ways. First, IMHA established a tradition of engaging all stakeholders in the process of defining research priorities via its consensus conference model – an integrated KT approach that helps bridge the disciplinary silos within IMHA's mandate. Second, IMHA was the first entity within CIHR to champion the end-of-grant KT tool – a program to accelerate translation of new knowledge acquired from funded research – in its strategic initiatives. This tool became an open competition funding opportunity in 2008. Third, IMHA is unique among CIHR Institutes in its citizen engagement activities, which are integral to KT at CIHR.
In 2005, IMHA launched the Knowledge Exchange Task Force (KETF), which comprises stakeholders committed to translating research knowledge to and for end users and helping to identify new research priorities. The work of KETF, which includes IMHA partner organizations and research ambassadors (patients/consumers), has focused on disseminating research findings, and developing and assessing lay-language summaries. Research ambassadors participate actively in the working groups of IMHA's IAB, workshops and conferences, including a partnership consultation held in Vancouver in March 2010. Selected research ambassadors have also worked on consumer commentaries for scientific journals, including a published editorial entitled Partnership in Action: An Innovative Knowledge-Translation Approach to Improve Outcomes for Persons with Fibromyalgia.Footnote 3 The KETF model was highlighted in the chapter Hearing Patients Voices in CIHR's Knowledge to Action: A Knowledge Translation Casebook (2008).
During the past five years, IMHA has partnered on the CIHR Knowledge Synthesis and Knowledge to Action RFAs, with a focus on encouraging IMHA researchers to increase work in the health services and population health domains. This has increased activity across IMHA's mandate, with four knowledge syntheses currently being conducted. IMHA has also supported the Cochrane Collaboration and recently established a Cochrane Corner on its website through which it promotes evidence-based decisions by providing links to syntheses in each of IMHA's strategic priority areas.
Other KT activities are described in the Outputs and Outcomes section.
Expanding partnerships
IMHA has become a focal meeting point for all research and KT partners in arthritis, bone, muscle, skin, oral health and MSK rehabilitation sciences. Since its inception, IMHA has built numerous internal and external funding partnerships, resulting in total partner contributions to research of $109.25 million, almost half of this since the last review (Table 1), an approximately two-fold leverage of IMHA's research and training investments.
Table 1: Leveraging of IMHA funding by partner contributions
| Year | Partners/Total Partner Contributions 2006–2010 | |
|---|---|---|
| 2006 | Institute of Aging (IA), Institute of Aboriginal Peoples' Health (IAPH), Institute of Genetics (IG), Institute of Infection and Immunity (III), Institute of Neurosciences, Mental Health and Addiction (INMHA), Institute of Nutrition, Metabolism and Diabetes (INMD), Multiple Sclerosis Society of Canada, Muscular Dystrophy Canada | $ 13,509,500 |
| 2007 | IG, INMHA, Amyotrophic Lateral Sclerosis Society, Muscular Dystrophy Canada | $ 1,716,666 |
| 2008 | Canada's Research-based Pharmaceutical Companies, IA, Institute of Cancer Research, Institute of Gender and Health, Institute of Human Development, Child and Youth Health (IHDCYH), III, INMD, INMHA, AUTO21, AstraZeneca Canada, Canadian Pain Society, Muscular Dystrophy Canada, Ontario Neurotrauma Foundation, Osteoporosis Canada, Public Health Agency of Canada, Sport Canada, Transport Canada | $ 21,319,597 |
| 2009 | CIHR knowledge translation and public outreach, IAPH, IA, Institute of Circulatory and Respiratory Health, IGH, IG, Institute of Health Services and Policy Research, IHDCYH, III, INMHA, INMD; Canadian Arthritis Network, Canadian Patient Safety Institute, The Arthritis Society | $ 7,311,500 |
| 2010 | The Arthritis Society | $ 600,000* |
| Total | $ 44,457,263 | |
Amounts are maximums, based on signed.
*Reflects memorandums of understanding completed to June 2010.
IMHA also is proactive in reaching out to solicit input on gaps and opportunities from national and international research funders and societies within its mandate. One of these is the Bone and Joint Decade (BJD). BJD, an international effort endorsed by more than 70 countries, was launched at the World Health Organization headquarters in Geneva, Switzerland in January 2000. As one of the lead Canadian partners of BJD and BJD Canada, IMHA hosted the Annual International BJD Conference, with the theme Standards of Care in November 2005. IMHA also supports the Young Investigators Initiative, a partnership between BJD U.S. and BJD Canada to mentor young investigators embarking on research careers. IMHA participated in the BJD Global Network Conference in Washington, DC in October 2009 in which IMHA's scientific director played a leadership role. With input from research leaders in the U.S., Japan, Australia, the UK and the Netherlands, she drafted the 2009 BJD position paper on gaps and opportunities in basic bone and joint research that included such key messages as the need to span research themes (at CIHR, these are biomedical, clinical, health systems and services, and social, cultural, environmental and population health) and promote multidisciplinary approaches, build multi-user platforms, increase capacity and establish methods to accelerate KT to and among multiple user groups.Footnote 7
IMHA held a non-governmental organization partner consultation in March 2010. Nearly 30 national and international charitable health organizations attended to learn about each other's current goals and to identify the priorities, gaps and opportunities required to advance oral, skin and musculoskeletal health and arthritis research and KT in Canada over the next five years. Outcomes included a mutual understanding of partner mandates, goals and programs, commitments to strengthen linkages and a list of actionable items for all partners to engage in and report on in the coming years.
Other ongoing partner activities are included in the Outputs and Outcomes and Going Forward sections.
Expanding training
IMHA's annual data collection and analysis document growth in training across all themes, primarily those with funding from grants and individual trainee awards. However, recognizing the need to build capacity in multidisciplinary research across all its areas, IMHA funded six Strategic Training Initiative in Health Research (STIHR) programs. Open competition and partners funded seven additional STIHRs within IMHA's mandate. Three renewal and two new STIHRs (now designated as training grants) were funded by IMHA and partners in 2009, for a total investment of $32.4 million in capacity building, with trainees across all of IMHA's focus and strategic research priority areas. Strategic decisions were taken to increase training capacity within IMHA's smaller foci by increasing the percentage of strategic initiative funding going to them (see Outputs and Outcomes section). To encourage new trainees to enter the field, IMHA has also provided studentships in mobility, musculoskeletal, oral, and skin health and other awards for undergraduate students to do research during the summer. One hundred and fifty-five students were funded between 2000–2009. A recent survey showed that 65% of them have gone on to further research or professional training in IMHA-related fields – career decisions many attribute to funding from IMHA.
Expanding ethics
IMHA has promoted interactions with CIHR's Ethics Office and ensured ethics values were incorporated into IMHA's 2008–2013 strategic plan, and IAB, IAB committees and working group meetings. IMHA recently championed an ethics decision-making framework that was piloted at its May 2010 IAB meeting. In 2009, IMHA's scientific director helped develop the draft CIHR guidelines for working with the private sector. Recognizing the importance of ethics and the role of the ethics designate to IABs, IMHA also contributed to the establishment of the annual CIHR Douglas Kinsella (IMHA's first ethics designate) Doctoral Award for Research in Bioethics.
Key Initiatives
Key Initiatives described in this section do not cover all the initiatives that IMHA has undertaken (see Figure 3, the IMHA Pipeline), but instead highlight IMHA's strategic responses to the unique needs and health challenges within the breadth of its mandate. The first initiative reflects the evidence-informed process used by IMHA to identify and address the general and specific gaps in overall capacity within IMHA's mandate; the process is ongoing but longitudinal data document that goals are being realized. The second was initiated prior to the first international review but came to its funding endpoint during 2005–2010. The third initiative was implemented during 2005–2010 and is ongoing. The outputs and outcomes of these initiatives demonstrate their different stages of development and maturation.
Initiative 1: Building and sustaining research activity and capacity across IMHA's six foci
The need
As outlined above, the socio-economic burden of chronic disease across IMHA's mandate is extremely large, with the burden of MSK conditions alone at the top of the list of the leading 20 diagnostic categories for the costs due to disease in Canada.Footnote 2 As well, there exist not only gaps, but also low capacity in research and KT to address these gaps across all IMHA areas.
IMHA's strategy
Given CIHR's position as the largest and one of the few funders of MSK, oral and skin research in Canada, IMHA made the explicit commitment to expand all six of its foci. As reflected in the IMHA Pipeline, workshops and consensus conferences were held to identify research gaps, and strategic initiatives were launched to redress them in all six foci. This was a nine-year process. No single research community was left out. As documented in the Outputs and Outcomes section, IMHA has succeeded in its goal to engage all of its research communities and their respective stakeholders, and to advance knowledge and build capacity in each focus. This has strengthened IMHA's community and positioned it to better address Canada's major chronic disease challenges (see Going Forward section).
Initiative 2: Osteoarthritis – from pain, disability and chronic disease to physical activity, mobility and health
The need
The impact of arthritis on Canadians is enormous. Health Canada's report Arthritis in Canada: An Ongoing Challenge (2003)Footnote 4 and The Public Health Agency of Canada's (PHAC) Life with Arthritis in Canada: A personal and public health challenge (2010)Footnote 5 establish the parameters of the issue. Arthritis remains common, costly and disabling. More than 4.2 million Canadians live with one or more arthritic conditions, and the number is expected to increase to 7 million by 2031. The most common arthritis is osteoarthritis (OA), which affects more than 10% of adult Canadians. It is a leading cause of pain and physical disability in Canada and a major public health challenge. It is noteworthy that IMHA is a member of PHAC's chronic disease surveillance committee and that most research underpinning the reports mentioned above is funded by CIHR.
IMHA's strategy
Recognizing the challenges, IMHA's first consensus conference was in OA, under the strategic priority of pain, disability and chronic disease. In this integrated KT model, approximately 200 delegates representing more than 30 national and international stakeholder groups – including basic researchers and clinician-scientists, professional organizations and partners, consumers and patient/public advocates, non-governmental organizations including the Arthritis Society, Canadian Arthritis Network (CAN), government and industry – helped develop research priorities to reduce the burden of OA. Five priority research questions were identified, all representing research gaps. For example, a significant gap identified by the patients/consumers at the conference was the need for a better understanding of the causes and treatment of pain and fatigue in OA. A significant outcome of the conference was the launch of an RFA and funding of OA New Emerging Teams (NET), in partnership with CAN. Outputs and impacts achieved include tools for earlier and better diagnosis, better measures of pain and transition of one NET to a PAMH team (see Outputs and Outcomes section).
Initiative 3: Disparities in oral health
The need
The oral health research community is small and many of its members and stakeholders are not well integrated with each other or other disciplines. Nevertheless, Canada's oral-health scientists are international leaders in such areas as oral infectious diseases, the biology of connective and mineralized tissues, biomaterials, neuroscience and pain. Less research is focused in the area of oral health disparities. Sixty to 80% of dental caries and most periodontal disease in Canada are experienced by disadvantaged and remote populations including Aboriginal peoples, the elderly and people who are cognitively or physically disabled.Footnote 6 In short, the very people who could benefit most from advances in dental care have poor access to treatment or can't afford it.
IMHA's strategy
IMHA organized two oral health research planning workshops that drew together a broad range of stakeholders. The workshops began laying the groundwork for a national oral health research strategy that would include research and training priorities. IMHA's oral health research Institute Advisory Board working group followed up with a series of additional consultations which, together with the Health Canada survey data, led to oral health disparities as the first priority. Thus, IMHA launched its Catalyst Grant in Disparities in Oral Health RFA in 2007. The grant was to support the planning and development activities of multidisciplinary and cross-theme research networks working to address disparities in oral health and oral health services among vulnerable populations. Our recently completed evaluation of the outcomes of the four teams funded documents notable successes (see Outputs and Outcomes section). The evaluation and ongoing SWOT analyses, however, highlight a need for the additional activities in oral health disparities and in oral health research generally that we have built into our future plans (see Going Forward section).
Outputs and Outcomes
Methodology
Outputs and outcomes reported are based on funding data provided from CIHR's Electronic Information System, data from IMHA's Micro-Impact Survey (MIS) tool, and bibliometric data provided by the Observatoire des Sciences et des Technologies (OST). It is worth noting some caveats and limitations of the datasets. Funding data are based on a keyword search of the CIHR funding database and validated through a subjective process. Reflecting the breadth and etiology of diseases and conditions under IMHA's mandate, projects may have affiliations with multiple institutes. OST used Medical Subject Headings (MeSH) searches to identify publications, and the databases searched may not cover all publications in IMHA's area. Average of relative citation (ARC) data, in particular, are incomplete for 2008. Countries were ranked based on total number of publications. Data reported as a percentage are rounded to the nearest whole number.
The MIS data summarize outcomes from 61% (64 of 105) and 51% (86 of 169) of IMHA strategic initiative-funded research grants (training grants, meeting, planning and dissemination grants, institute community support awards, or grants less than $15,000 were excluded). Data compare outputs across two funding timelines (2000–2005 and 2005–2010). There is no overlap between the two time periods. (The first includes grants that received the first funding amount up to fiscal year-end March 2005 and the second starts at fiscal year start April 2005. Because grants with end dates in 2010 or later were not surveyed, 2005–2010 outcomes are underestimated. Note that the response rate was 57, 62, 90, 70, 60 and 25% for grants related to arthritis, bone, muscle, musculoskeletal (MSK) rehabilitation, skin and oral focus areas in 2000–2005 and 47, 40, 52, 64, 54 and 86% in 2005–2010. Consequently, differences in response rates by foci should be considered when examining numerical data – e.g., number of publications or number of students trained. Finally, since some research projects can be classified as related to more than one focus area, there will be overlap (although minimal) in some data points.
Initiative 1: Building and sustaining research activity and capacity across IMHA's six foci
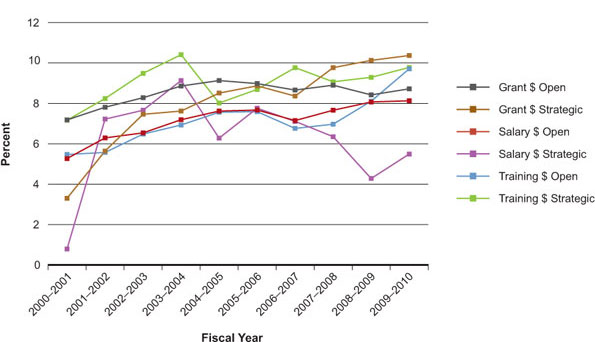
The percentage of total annual CIHR expenditures in IMHA-relevant open and strategic grants and training awards has increased over time, with equal or slightly greater contributions from strategic funding, except for salary awards (Figure 4). In IMHA-relevant areas, funding data show that the open and strategic funding to grants (salary and training awards excluded) was $17.76 million and more than $1 million in 2000–2001, respectively, and grew to $40.83 million and nearly $24.8 million in 2009–2010, respectively. Similar patterns are observed in strategic contributions to salary and training. The percentages display strategic and open percentage contributions against total CIHR expenditures, which include IMHA-relevant and non-relevant areas. Values are calculated only within a particular year thereby somewhat obscuring information about growth. In this context, despite the reduced percentage of strategic contribution towards salary awards between 2007 and 2010, salary funding to IMHA-related researchers grew considerably more than in the open competition when 2000–2001 funding data are used as baseline.
Figure 4: Percentage of total CIHR expenditures invested annually in IMHA-relevant grants, training and salary awards
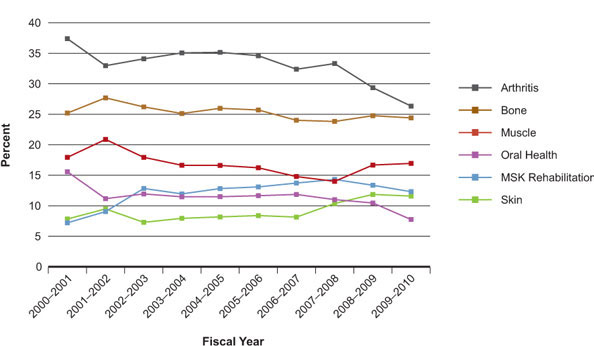
IMHA's arthritis and bone foci were initially and remain the largest in terms of funding compared to MSK rehabilitation, muscle, skin and oral health (Figure 5). The percentages are focus-specific percentage contributions against total CIHR expenditures in IMHA-relevant areas. The percentage of CIHR funding in IMHA's foci has remained relatively stable over the last 10 years, with moderate decreases in arthritis and oral health, slight decreases in bone and muscle, and slight increases in MSK rehabilitation and skin in 2009–2010 relative to 2000–2001. CIHR investment in all six foci except oral health has grown, relative to the 2000 baseline, more than the growth of total CIHR expenditures.
Figure 5: Percentage of CIHR expenditures invested annually in IMHA's focus areas
Recognizing the strengths of its arthritis and bone communities, IMHA made the decision to direct more of its strategic initiative budget in the last five years to building capacity and activity in the smaller foci of muscle, MSK rehabilitation, skin and oral health. Fifty-three percent (56 of 105) of IMHA strategic-initiative funded research grants between 2000−2005 were related to the latter four areas: 60% (63 of 105) were arthritis or bone related. In 2005–2010, 65% (110 of 169) of IMHA strategic-initiative funded research grants were related to MSK rehabilitation, muscle, skin or oral health; 45% (76 of 169) were related to arthritis or bone. As shown below, this has increased research activity and capacity in the four smaller foci.
Advancing knowledge
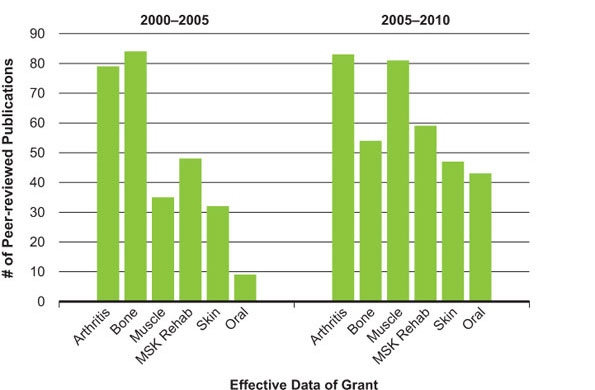
In the 2000–2005 period, IMHA-funded principal investigators (PIs) in the MSK rehabilitation, muscle, skin and oral health areas reported fewer contributions to the peer-reviewed literature than those in arthritis and bone. In the last five years, however, contributions to the peer-reviewed literature by the four smaller foci have increased (MIS data, Figure 6). Overall, 97% of all IMHA-funded PIs reported at least one publication resulting from their 2005–2010 research grant, up from 94% in 2000–2005; 26% and 15% of PIs also reported at least one book contribution or technical report each, up from 20% and 14%, resulting from grants funded in 2000–2005.
Figure 6: Number of peer-reviewed publications obtained or expected from IMHA strategic-initiative research grants by focus area
Bibliometric analysis of PI publications funded by CIHR (including IMHA strategic-initiative funded) in all areas relevant to IMHA's mandate documented substantial growth in contributions from 0.9% of the world's papers in 1997 to 1.4% in 2008. CIHR-funded PIs contributed to 19% of Canadian papers in IMHA-related areas in 1997 and 25% in 2008. These are averages of all IMHA foci, with some foci much higher (e.g., arthritis) and some lower (e.g., oral health). Nevertheless, researchers funded by IMHA's strategic initiative budget have seen slightly greater increases in growth of contributions to Canadian papers compared to all PIs funded by CIHR in IMHA-related foci (Figure 7). These researchers are also publishing more papers with international collaborators, i.e., 30% in 1997 had at least one international author on an article compared to 40% in 2008 (OST data).
The impact of Canada's output within IMHA-related foci is evident from the average of relative citations (ARC), a standardized measure of citations: Canadians are more cited (ARC = 1.18) than the other top-five producing countries (Table 2, "All"). The citation scores of IMHA-related papers published only by CIHR-funded PIs are higher across all of our foci compared to the publications of all Canadian researchers, as well as those of all of the other top five producing countries, except the U.S. for oral and muscle areas. Thus, CIHR-funded researchers in IMHA-related foci are among the most cited and their contributions to world publications pools have been increasing.
Figure 7: Percentage growth (relative to 1997) in contributions to total yearly Canadian papers in IMHA-related areas by CIHR and IMHA strategic initiative-funded PIs
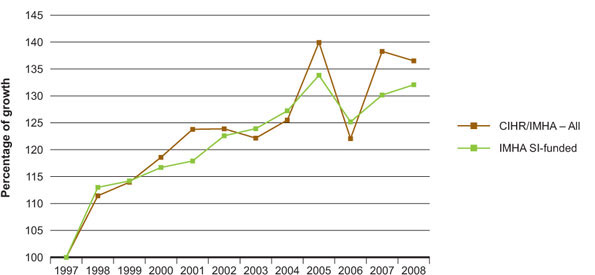
Table 2: Average of relative citation (ARC) values between 2003–2008 of IMHA-related research articles in the top six producing countries, and ARC values for publications of PIs funded by CIHR
| CIHR | Canada | U.s. | UK | Germany | Japan | France | |
|---|---|---|---|---|---|---|---|
| Arthritis | 1.4 | 1.31 | 1.34 | 1.38 | 1.07 | 0.82 | 1.16 |
| Bone | 1.44 | 1.31 | 1.3 | 1.24 | 1.03 | 0.79 | 1.04 |
| MSK Reha | 1.62 | 1.38 | 1.2 | 1.11 | 0.93 | 0.72 | 0.97 |
| Muscle | 1.23 | 1.14 | 1.27 | 1.23 | 1.11 | 0.8 | 1.01 |
| Oral | 1.21 | 1.13 | 1.24 | 1.05 | 1.12 | 0.84 | 1.08 |
| Skin | 1.48 | 1.46 | 1.3 | 1.34 | 1.18 | 0.82 | 1.07 |
| All | 1.35 | 1.18 | 1.17 | 1.17 | 1.09 | 1.01 | 0.91 |
An ARC value above 1.0 for a country means that, on average, the country's publications by researchers in that field are cited more often than the world average. The "All" number is calculated separately and includes all IMHA-related publications, i.e., it is not the average of the focus areas alone.
Capacity building
Capacity building in IMHA-relevant research foci entails not only funding more researchers, but also training more graduate students and postdoctoral fellows. CIHR's open and strategic contributions to training in IMHA-relevant research areas have increased considerably since 2000 (Figure 4). Specifically, in the last five years, 541 training awards were funded by open and strategic funding in IMHA-relevant areas, up from 237 in the 2000–2005 period.
The number of graduate students and postdoctoral fellows trained on strategic initiative-funded projects in IMHA's previously under-represented foci of muscle, MSK rehabilitation, skin and oral increased in the 2005–2010 period (Figure 8). Similar increases were observed in undergraduate student training, with 36% and 69% of PIs reporting training at least one undergraduate student on strategic initiative grants between 2000–2005 and 2005–2010, respectively. Thus, there is a trend towards increased training within the previously under-represented areas. This reduces the disparities observed in the 2000–2005 period.
Figure 8: Number of graduate students trained on strategic initiative-funded research grants
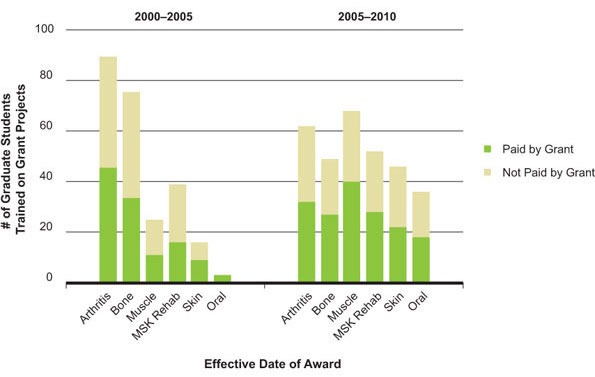
Data reflect training on research grants and not training awards.
Informing decision making
Results of research funded by IMHA's strategic initiative budget are disseminated to audiences not only in peer-reviewed publications, but also directly to health professionals, policy makers, news media, the public and patients. Disseminating research in this manner may accelerate the uptake of strategic initiative-funded research into policy and practice. No major differences were observed between the two time periods surveyed. However, since more PIs were IMHA-funded in the 2005–2010 period, more outcomes related to information dissemination are expected to occur. One PI (Janet Pope, Saint Joseph's Health Centre in London, Ontario) made the following observation in the 2008 Walkerton Health Study about the value of disseminating research on the long-term risk of chronic arthritis following campylobacter infection: "We informed the Walkerton community via a newsletter of our research (and other research) due to the contaminated water and its outcomes on arthritis. I was asked to write a prestigious Current Opinion review in reactive arthritis mostly due to this work."
Health and health system/care impacts
Although it is difficult to measure the impact of funding on health systems in the short term, MIS data revealed that many IMHA strategic initiative-funded researchers are committed to contributing beyond the scientific literature. Roughly half of strategic initiative-funded PIs reported that they developed (or were developing or trialing) new products or that their results were translated (or planned to be translated) into clinical or medical practice. Another 39% and 34% reported that their research results were already or would be cited in clinical guidelines or health policy documents in the 2000–2005 and 2005–2010 periods, respectively. Despite no major differences in the two time periods, more PIs were IMHA-funded in the 2005–2010 period and therefore more such outcomes related to health systems impact are expected to occur.
Economic impacts
A trend towards increased disclosures and patenting was reported by IMHA strategic initiative-funded PIs. The percentage of PIs reporting that a patent was assigned remained steady at 5% during the time periods 2000–2005 and 2005–2010. However, during the time period 2005–2010, 16% of PIs reported that they had applied for or were writing patent applications. This is up from 13% reported during the 2000–2005 time period.
Collectively, the data indicate that IMHA has met the goal of its first strategic plan to build capacity, and advance and translate new knowledge with measurable outputs and impacts in all six of its foci, with notable increases in its smaller areas. Our data also indicate that we are on target for the goals of IMHA's second strategic plan.
By expanding and strengthening Canada's IMHA-relevant research community, particularly its smaller areas, IMHA is ensuring the availability of new knowledge across its mandate and its dissemination for changes to policy, improvements to health systems and care, and commercialization.
Initiative 2: Osteoarthritis New Emerging Teams – from pain, disability and chronic disease to physical activity, mobility and health
IMHA, with its partner CAN, funded three OA New Emerging Teams (NETs) in 2003. In 2004, a fourth OA NET was funded via an IMHA quality of life NET. Collectively, the NETs covered all themes and all of the questions and gaps identified in the OA consensus conference.
IMHA commissioned RAND Europe to survey the OA NETs, including the PIs, co-PIs and co-applicants. The report8 documents the key role OA NETs played in advancing knowledge, building capacity and informing policy over five years. The publications resulting from these NETs are part of the arthritis data described below.
Advancing knowledge
Canadian researchers published 2,416 arthritis articles between 2000–2008, tying with the U.S. and the UK with an average of relative citations value of ~1.33 (Figure 9). IMHA strategic initiative-funded researchers alone contributed to 41% of all arthritis papers by Canadian researchers in 2008.
Figure 9: Specialization index and average of relative citations for top 10 countries publishing in arthritis, 2000–2008
Informing decision making, health and health system/care impacts, economic impacts
Beyond publications in the peer-reviewed literature, OA NETs produced other outcomes important to research, health care and health care costs, commercialization and policy. In total, every OA NET produced at least one new research tool with a total of 27 distinct tools reported,Footnote 8 including:
- An animal model of OA
- A patient survey
- Composition (formulation) for drug delivery
- Potential new drug targets
- Patient and physician decision support tools including newsletters and videos
Two OA NETs also reported patent applications and gene therapy agents that are in animal trials (i.e., an early stage of development).
The total number and categories of tools reported give a snapshot of important quantifiable outcomes, but a few more specific examples are equally compelling. One relates to the need for better, earlier diagnosis and treatment of OA that can be initiated before massive joint destruction is evident on radiographs. This tool is crucial to reduce the socio-economic burden of OA but remains a challenge. Jolande Cibere from the Esdaile OA NET won a Young Innovator Award in 2005 from the Networks of Centres of Excellence for research that led to development and copywriting of a standardized clinical knee examination for early OA diagnosis and prevention. Such an exam was lacking prior to her work. This knee exam is now being used in the U.S. National Institutes of Health (NIH) Osteoarthritis Initiative, a collaboration with industry to develop a public repository of OA patient data.
Cibere and colleaguesFootnote 9 have more recently asked about the association of 10 biomarkers with knee OA and, specifically, whether biomarker levels are associated with the pre-radiographic or radiographic stage of OA in a population-based study. The team showed that several urinary and serum biomarkers, taken together, are associated with pre-radiographic OA and an increased risk of developing radiographic OA, making them potentially useful diagnostic tools for early pre-radiographic disease.
This study is unique and important not only for being the first study to measure a wide range of biomarkers and the first to do so in subjects with pre-radiographic, magnetic resonance imaging-proven OA, but also because the results are based on the evaluation of a population-based cohort and hence can be generalized to the Canadian population. Through pharmacy-based cohort studies led by Carlo Marra, this team also determined that they can establish large cohorts where new assessment and intervention tools can be tested. The results of their first study (PhiT-OA) are empiric evidence of whether this multidisciplinary strategy can improve real-world outcomes for knee OA. The team is negotiating with the government of British Columbia to improve outcomes in OA by using PhiT-OA as the model for similar randomized control trials in communities throughout BC. This team also has intellectual property rights for Research Measure: Social Role Participation Questionnaire.Footnote 10
Another example is the Hawker OA NET that, among other outcomes, developed and published a new pain measure, the Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP), for hip/knee OA. The tool is suitable for use as an outcome measure in clinical trials of OA disease-modifying agents and to evaluate the need for total joint replacement of the hip and knee. Thus, it assists in prioritizing patients on the waiting list for hip and knee replacement surgery. The ICOAP has been translated into a number of languages and is being evaluated further in an international collaboration led by Hawker in large epidemiologic cohort studies, including the NIH Osteoarthritis Initiative and industry- and peer-reviewed clinical trials.Footnote 11,Footnote 12
Capacity building
All OA NETs achieved another program goal: acquiring additional funding in open and strategic competitions.Note en bas de page 8 Most expanded their NET funds into more than one additional funding mechanism and two have grown into teams that have attributed their ability to do so to the OA NETs. One team grew into the Community Alliances for Health Research and Knowledge Exchange on Pain. Another succeeded in IMHA's first initiative to increase research and KT in Physical Activity, Mobility and Health, the flagship priority of the Institute's second strategic plan. Among four PAMH teams announced and funded by IMHA and its partners in July 2010 was the CIHR team in Investigations of the Mobility, Physical Activity and Knowledge in Hip Pain. This multidisciplinary team is investigating how the repetitive hip flexion involved in sports like hockey, soccer and bicycling and deformities of the hipbone combine to cause pain and eventually OA.
Other important outcomes of the OA conference were the funding of multiple STIHRs with strong OA training components. The OA conference also made apparent the importance of integrating the work of all stakeholders involved in the research and care of those with arthritis. IMHA was therefore a founding member of the Alliance for the Canadian Arthritis Program (ACAP) with the Arthritis Society and the Canadian Arthritis Network (CAN). ACAP now includes representatives from more than 30 stakeholder organizations, including the Canadian Rheumatology Association, Canadian Orthopaedic Association, Canadian Arthritis Patient Alliance, Canadian Alliance of Pediatric Rheumatology Investigators, Cochrane Collaboration and the Public Health Agency of Canada. ACAP provides a forum for all stakeholders to work together toward achieving solutions to outstanding national arthritis care needs such as access to appropriate treatments. It also provides a single message to government and industry in matters relating to arthritis health policy (see Going Forward section).
The OA NET tool provided unique advantages, demonstrating that:
- the complexities of chronic disease are best tackled through a comprehensive, multidisciplinary team approach
- trainees exposed to a multidisciplinary team approach are better prepared and more competitive for the next phase of their career
- outputs include knowledge advancement and translation with marked health systems/health care and commercialization impacts
Initiative 3: Disparities in oral health
In 2007, IMHA launched an RFA and funded four catalyst grants to facilitate the building of networks that advance and translate knowledge to address disparities in oral health (DOH). As summarized in data below, acquired using the MIS tool, the strategic program was highly successful in meeting its objectives and is having important impacts that would very likely not have resulted from oral health research funded solely via an open competition process.
Capacity building
The program successfully promoted the building of multidisciplinary, multi-sectoral teams to address oral health disparities in vulnerable populations in Canada. An average of 7.8 co-PIs and co-applicants were involved in each of the four projects and the PIs reported an average of 6.3 collaborations resulting from each grant. Such networking was likely crucial to the grant outcomes summarized below as well as expected future outcomes.
Advancing knowledge and informing decision making
Not only did the DOH grants produce a large number (21) of publications, but results were also disseminated to a broad array of stakeholders and knowledge users. DOH researchers interacted with health care professionals, health service decision makers and individuals representing vulnerable groups, government bodies interested in developing oral health policies and professionals in community-based dental clinics. The reported interactions with health care stakeholders are being translated into processes that will aid in the development of national and province-wide strategies to reduce oral health disparities.
Health and health system/care impacts
The four teams funded by the catalyst grants have formed a larger network of teams for sharing information and best practices. IMHA's original oral health workshops, ongoing consultations and the research resulting from the DOH program provided the impetus for an IMHA co-sponsored workshop in DOH held by the Canadian Academy of Health Sciences (CAHS). This led to a CAHS-commissioned assessment on improving access to oral health care for Canadians. Chaired by Paul Allison (a PI of one of the DOH catalyst grants), the assessment panel includes individuals from a wide variety of academic and non-academic backgrounds, whose expertise spans different elements of dentistry, including dental therapy, dental hygiene, dental licensing bodies, dental public health and academic dentistry, plus other non-dental fields, including health services, health law, health economics, health policy, geriatrics and pediatrics. The panel includes international experts in dental services delivery from the U.S. and the UK. The panel's task is to make recommendations that will improve access to oral health care services, particularly for vulnerable groups in Canada. The work of the panel is financed through grants from Canadian dental faculties, several research granting agencies, including IMHA, a dental licensing body and donations from the private sector. The panel of 14 first met in two separate groups in May and June 2010 and the core work of the panel is now well underway. The broad lines of the report's content are decided and detailed material is now being amassed. The panel is expected to meet in the winter and in the spring of 2011. Publication of the report is expected in approximately a year.
The DOH program met its objectives to support the building of multidisciplinary, multi-sectoral teams and networks to advance and translate knowledge that will improve oral health and oral health care of vulnerable Canadian populations.
Going Forward
CIHR's strategic plan, Roadmap, provides clear direction for the next several years. IMHA's second strategic plan and initiatives dovetail strongly with Roadmap and, as evidenced by the community building, capacity building, increase in multidisciplinary approaches and demonstrable impacts achieved over the last 10 years, IMHA is delivering on all four strategic directions of Roadmap. IMHA will be part of the solution to the chronic disease burden that is threatening individual and population health and the health care system in Canada.
Musculoskeletal conditions and arthritis
Bone and joint diseases and conditions must continue to be central in IMHA's research and KT strategy. IMHA has sought closer relationships with its government agency partners, an outreach that has resulted in IMHA now being represented on two important federal government policy initiatives under its mandate: PHAC's Chronic Disease Surveillance Advisory Committee and the Health Portfolio Physical Activity Guidelines revision group of PHAC.
IMHA participates as a founding member of the Alliance for the Canadian Arthritis Program (ACAP), which now integrates more than 30 stakeholder groups involved in the research and care of those with arthritis. But this landscape is changing: the Canadian Arthritis Network (CAN), the third largest funder of arthritis research in Canada after IMHA and the Arthritis Society, will come to the end of its mandate in 2012, having been funded for the maximum duration possible. IMHA championed meetings of these major arthritis funding agencies for forward planning and, together with CAN, the Arthritis Society and ACAP, IMHA is funding a domestic and international environmental scan. The first phase will be completed before the end of 2010 and will help inform a synergistic national arthritis research funding strategy. Without IMHA, this essential data gathering and planning exercise would not have happened.
A companion piece to the environmental scan is development of a national framework or action plan for research, KT and implementation of standards of arthritis prevention and care. A landmark Summit on Standards in Arthritis Prevention and Care, sponsored by IMHA and its ACAP partners, led to standards detailing the minimal acceptable levels for arthritis care and prevention irrespective of where someone resides in Canada; this work formed the framework for ongoing activities. Over the last year, ACAP and its partners have sponsored a data analysis tentatively entitled Looking Forward: Impact of Arthritis 2010–2040, a report geared towards modeling outcomes of interventions for OA and inflammatory arthritis. The report is being finalized and its release is imminent. Among other deliverables are a robust communications plan. The plan will end Phase I and launch Phase II of a detailed framework for determining the actions and resources necessary to prevent all forms of arthritis and improve the care of Canadians who have arthritis. Phase III will be for implementation: executing the strategies, measuring results and adjusting the approach.
IMHA recently outlined in detail its alignment with the CIHR Roadmap's Strategy for Patient-Oriented Research (SPOR). SPOR offers a vehicle by which IMHA and its national and provincial partners can deliver on opportunities in arthritis research and care. It also offers opportunities in other chronic MSK conditions, including osteoporosis, and implementation of Osteoporosis Canada's 2010 Practice Guidelines for the Diagnosis and Management of Osteoporosis in Canada.Footnote 13 IMHA participated in the official launch of the guidelines in late October 2010, where we acknowledged the CIHR-funded research that underpins the guidelines and reiterated IMHA's commitment to helping implement them. Following a highly successful Bone Health Consensus Conference in late fall 2009, which followed the model of the OA conference in bringing together key stakeholders and partners, IMHA launched a request for applications (RFA) and recently announced funding of 16 catalyst grants in bone health. These will enable planning and development of teams in bone health, for which an RFA will be launched in late 2010. We anticipate that these activities will accelerate, along with SPOR activities, new research and KT not only to better diagnose and treat osteoporosis, but also to prevent it in future.
The need for an oral health research agenda
As noted in the Outputs and Outcomes section, IMHA is co-funding the assessment commissioned by CAHS on disparities in oral health and health care. This, and data generated from the disparities in oral health catalyst grants, contribute directly to the Roadmap priority to reduce the health care inequities faced by Aboriginal peoples and other vulnerable populations. IMHA will play a convenor role in bringing together oral health services researchers, practitioners, consumers, the relevant policy makers and other stakeholders to improve oral health.
IMHA's consultations and evaluation activities have also uncovered significant areas of concern for oral heath research in Canada. Oral health research remains the smallest of IMHA's six foci and, in spite of notable strengths, uniquely among the foci has grown less than the overall CIHR average from 2000–2010. The dental science peer-review committee was disbanded in 2009 due to low application pressure and, while the related applications have been accommodated in a variety of other discipline-related committees, concerns remain that certain oral health research topics may be falling between the cracks, and that whole segments of oral health research may be in jeopardy. Based on the data and broad-based discussions of IMHA's working group on oral health research, IMHA is leading a strategy group to bring together deans of dental faculties and schools, the Canadian Association of Dental Research and the Canadian Dental Association to develop an oral health research strategy for Canada, a role that only IMHA can ensure continues to develop.
Inflammation in chronic disease
IMHA believes that inflammation research is the key to new discoveries for improved health and reduction of the burden of chronic disease. Inflammation is an essential, natural response to acute tissue damage and is tightly regulated; its dysfunction contributes to imbalances in tissue homeostasis and to a plethora of disorders such as autoimmune diseases (e.g., arthritis, psoriasis, inflammatory bowel diseases), asthma, atherosclerosis, obesity, diabetes, periodontal disease and tooth loss, and transplant rejection. In fact, there is growing evidence that low-grade inflammation may contribute to a variety of local and systemic metabolic changes that underlie many chronic diseases including cancer. Additionally, physical activity has demonstrable anti-inflammatory effects in a number of chronic diseases.
Inflammation research is supported in the CIHR open grants competitions, and in the research funding programs led by other organizations. However, research in inflammation is siloed across particular chronic diseases and conditions, making recognition of common pathways, common biomarkers and potentially useful common interventions for inflammation management difficult. To address these gaps, IMHA is leading, in partnership with at least four other CIHR Institutes and external parties, a new initiative entitled Inflammation in Chronic Disease. The initiative crosses all three of IMHA's strategic priorities and continues the evolution of cross-focus multidisciplinary approaches that IMHA has championed successfully. The initiative is still in planning stages, but in keeping with IMHA's collaborative integrated KT planning model, a consensus conference of major stakeholders will help identify and prioritize gaps, research questions and opportunities, ultimately leading to appropriate RFAs (e.g., for multidisciplinary teams).
Future success
IMHA is a central player in Canada with regard to research and KT for musculoskeletal, oral and skin health. IMHA will drive progress towards meeting its strategic goals by continuing to monitor and sustain the pipeline of excellent research across all themes and foci within its mandate. It will provide leadership through sustained and new partnerships, and convene stakeholders to identify knowledge gaps and help implement solutions. The Institute will further develop international relationships and make progress toward its mission of reducing the burden of chronic disease in Canada.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
IMHA specific
| ACAP | Alliance for the Canadian Arthritis Program |
| BC | British Columbia |
| BJD | Bone and Joint Decade |
| CAHS | Canadian Academy of Health Sciences |
| CAN | Canadian Arthritis Network |
| DOH | disparities in oral health |
| IAB | Institute Advisory Board |
| ICOAP | intermittent and constant osteoarthritis pain |
| KETF | Knowledge Exchange Task Force |
| KT | knowledge translation |
| MeSH | U.S. National Library of Medicine Medical Subject Headings |
| MIS | Micro-Impact Survey |
| MSK | musculoskeletal |
| NET | New Emerging Team |
| NIH | National Institutes of Health |
| NSERC | Natural Sciences and Engineering Research Council |
| OA | osteoarthritis |
| OST | Observatoire des Sciences et des Technologies |
| PAMH | physical activity, mobility and health |
| PDCD | Pain, Disability and Chronic Disease |
| PHAC | Public Health Agency of Canada |
| PhiT-OA | empiric test of whether this multidisciplinary strategy can improve real-world outcomes for knee OA |
| PI | principal investigator |
| RFA | request for applications |
| SPOR | Strategy for Patient-Oriented Research |
| STIHR | Strategic Training Initiative in Health Research |
| SWOT | strengths, weaknesses, opportunities and threats |
| TIRR | Tissue Injury, Repair and Replacement |
- Date modified: