CIHR Internal Assessment - Report for the 2011 International Review
Part 3: CIHR's Evolving Role in Canada's Science and Technology Landscape
Canada's science and technology strategy and the Government of Canada's priorities
Canada's 2007 Science and Technology Strategy, called Mobilizing Science and Technology to Canada's Advantage,19 outlines three Canadian advantages: an entrepreneurial advantage, a knowledge advantage and a people advantage. It also outlines four priority areas: health and related life science and technologies; environmental science and technologies; natural resources and energy; and information and communication technologies. In September 2008, the Government of Canada accepted the recommendations of the Science, Technology and Innovation Council (STIC) that defined detailed sub-priorities. For health and related life science technologies these are: regenerative medicine, neuroscience, health in an aging population, biomedical engineering and medical technologies. In recent competitions of the Canada Excellence Research Chairs, Networks of Centres of Excellence and Centres of Excellence for Commercialization of Research, Industry Canada has imposed that Tri-Council research funding be oriented towards these priority areas.
CIHR has also taken into account these sub-priorities in its 2009–2014 strategic plan. In addition, it responded to priorities of the Minister of Health and to emerging health threats in launching specific requests for applications. Examples include: the rapid-response SARS research initiative and consortium in 2003; the wait-times studies of 2005 to inform provincial and territorial ministry of health decisions on benchmarks; the 2006 Pandemic Preparedness Strategic Research Initiative; and research on H1N1 and relevant public health and health care system interventions in 2009. In response to the recent radioisotope shortage, CIHR launched the Initiative in Alternative Radiopharmaceuticals for Medical Imaging, followed by the formation of a clinical trials network for medical imaging to accelerate translation of research discoveries on isotopes and imaging technologies into clinical practice. Most recently, at the request of the Minister of Health, CIHR, in collaboration with the Multiple Sclerosis Society of Canada, convened a meeting of leading North American researchers to provide advice on the appropriateness of launching a pan-Canadian therapeutic trial on venous angioplasty as a treatment for multiple sclerosis.
Changes in the nature and location of Canadian health research
CIHR's emphasis on multidisciplinary collaboration as the way to advance knowledge about the complex problems of health in society has helped to accelerate the structural changes in the Canadian research environment already under way at the end of the last century. A key evolution has been the rise of the academic health sciences centres and associated teaching hospital-based research institutes. Although each is affiliated with a university, these institutions are independently governed with respect to research organization, structure and priorities. The Association of Canadian Academic Healthcare Organizations noted that, in 2006, member institutions received more than $3 billion in research funding and almost 80% of public funding for health research20 and, in 2008, ran two competitions exclusively for research hospitals, spending $492 million.
Less confined by the traditional disciplinary structure of universities, academic health care organizations have more easily adopted interdisciplinary working arrangements – as well as making the translational link between bench and bedside – by combining research and patient care within the same organization. A recent report by the National Task Force on the Future of Canada's Academic Health Sciences Centres21 proposed that they form the nucleus of an Academic Health Sciences Network, "created by health sciences universities, academic health care organizations and other provider organizations with the goal of improving patient and population health outcomes through mechanisms and structures that develop, implement and advance integrated health services delivery, professional education, and research and innovation." While challenging the traditional role of universities as the leaders of the research enterprise, this model has the advantage of facilitating translational research and subsequent KT, and assembling regional communities of interest that are well placed to interact with the public and policy makers.
There has also been a shift of CIHR-funded research into community-based organizations that exist entirely outside the academic sphere, including those that serve Aboriginal peoples and those that provide care and education services to defined patient groups, in particular to HIV/AIDS community organizations. Further investment in Aboriginal peoples' health and a greater emphasis on primary health care research will accelerate this trend.
Evolution of Canada's health research workforce
CIHR-supported researchers (including trainees with studentships or fellowships)22 have increased from 5,370 in 2000–2001 to 13,790 in 2009–2010. Support for themes 3 and 4 has particularly increased. For example, the number of students with CIHR awards working in these two theme areas increased from 56 in 2000–2001, or 6.5% of the total, to 485 in 2009–2010, or 25% of the total. In 2009–2010, CIHR supported health researchers and trainees at 332 research institutions in every province of Canada. The regional distributions of funding and funded institutions in 1999–2000 and 2009–2010 are shown in Figure 10. Many of the newly funded institutions do not have a medical school, but have strengths in the social sciences that contribute to the broadened mandate of CIHR, such as the Universities of Northern British Columbia,23 Regina, Windsor, le réseau de l'Université du Québec and Acadia University.
Figure 10A: Regional distribution of funding in 1999–2000 (MRC) and 2009–2010 (CIHR)
Figure 10B: Number of research institutions 1999–2000 and 2009–2010

Source: CIHR funding database.
Direct payments are excluded in the figure above.
The Regional Partnerships Program has been created to assist small provinces in building their research capacity. It funds applications from the six participating provinces (Saskatchewan, Manitoba, New Brunswick, Prince Edward Island, Nova Scotia and Newfoundland) that fall just below the funding cut-off but are highly rated in CIHR's open competitions and are also relevant to priorities identified by each province. These applications are funded on a 50-50 basis between CIHR and provincial sources. Table 4 provides provincial comparisons of CIHR funding.
The absence of any CIHR funding allocated to the three territories does not mean that northern health research is neglected. Since 2000, CIHR has invested in excess of $46 million in more than 100 northern health research projects, involving more than 30 institutions.
Table 4: Provincial comparisons
| Province | Increase in Funding, 1999–2000 (MRC) – 2009–2010 (CIHR) | Per Capita CIHR Funding, 2009–2010, $ |
|---|---|---|
| Quebec | 163% | 29.69 |
| Ontario | 197% | 26.03 |
| Nova Scotia | 267% | 26.03 |
| British Columbia | 345% | 24.91 |
| Alberta | 104% | 19.90 |
| Manitoba | 126% | 16.24 |
| Saskatchewan | 266% | 9.96 |
| Newfoundland and Labrador | 91% | 7.00 |
| Prince Edward Island | 340% | 4.19 |
| New Brunswick | 1,159% | 1.46 |
Preparing for tomorrow: research trainees
Canada's science and technology strategy emphasizes a "people advantage" and the need to grow the number of highly qualified personnel involved in the knowledge economy. Historically, Canada has a low rate of PhD production relative to its spending on research (Figure 11), especially in the sciences and technology, where it ranks 22nd among OECD countries for the percentage of PhDs awarded in the sciences.24 Accordingly, recent Tri-Council programs have focused on research trainees, featuring stipend levels competitive with additions to other postgraduate employment options.
Figure 11: PhDs awarded per million expenditures on R&D in the higher education sector
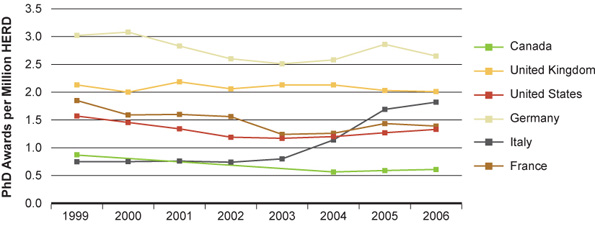
Source: OECD data reproduced in Performance of the UK Research base, 2009.
HERD: Higher Education Research and Development
Through the new Tri-Council programs and its own longstanding trainee programs, CIHR now supports approximately 4,800 graduate students and 2,000 postdoctoral fellowships through three different funding schemes (Table 5). In 2009, the Government of Canada provided three-year, non-renewable funding for 200 more doctoral and 800 more master's level Frederick Banting and Charles Best Canada Graduate Scholarships. The announcement in the federal government's Budget 2010 of a prestigious new Tri-Council postdoctoral awards program, the Banting Fellowships, will allow CIHR to offer 20 to 25 more postdoctoral fellowship awards annually.
There is no comprehensive source of information about the total number of health research trainees in Canada, because numbers are reported by university departments, not by subject of study, and research relevant to human health can be conducted in departments ranging from anthropology to zoology, neither of which are classified as health or medical departments. However, to the extent that health-related disciplines can be identified, there have been recent increases in enrolments at Canadian universities: MSc enrolments increased from 5,820 in 1999 to 9,660 in 2006 (the latest year for which data are available), and PhD enrolments from 1,614 to 2,487.25
Trainees can be supported by CIHR in three ways: with an individual award, through a CIHR Strategic Training Initiative in Health Research (STIHR) or as a graduate or post-graduate student paid from the supervisor's CIHR operating grant, the most frequent form of support.
CIHR supports more than two-thirds of health research graduate students in Canada, with the others supported by health charities, provincial health research organizations, institutional teaching stipends and other awards. Undergraduate students are supported as summer or co-op students (Table 5).
Table 5: Estimates of the total number of trainees supported directly and indirectly by CIHR and other sources, 2008–2009
| Level of Training | |||||
|---|---|---|---|---|---|
| Undergraduate | Master's | Doctoral | Postdoctoral Fellows (PDF) | Other | |
| CIHR Personnel award | 281 | 373 | 1,005 | 839 | 70 |
| STIHR | 193 | 227 | 410 | 257 | |
| Operating grants | 2,000 | 1,600 | 1,100 | 900 | |
| CIHR Total | 2,474 | 2,200 | 2,515 | 1,996 | |
| Estimates of the number of trainees supported directly by awards from health charities and provincial health research agencies | |||||
| All programs | 365 | 474 | 411 | 503 | |
| Estimates of the number of trainees in health research supported directly by the other two federal granting agencies | |||||
| NSERC | 1,210 | 461 | 587 | 112 | |
| SSHRC | 52 | 120 | 17 | ||
| Grand Total | 4,049 | 3,187 | 3,633 | 2,628 | |
Source: Begin-Heick, N. 2010 "An environmental scan of the support for training in health research in Canada".
A radical departure from the traditional support for research trainees was the introduction in 2003 of the CIHR STIHR Program, which provides a six-year grant to a group of mentors to organize an interdisciplinary training program. The grant is used to recruit and support trainees, for trainee exchanges between participating institutions and for developing educational materials. Following a positive evaluation of this program, a second round of 50 STIHR grants was jointly funded from institute and global budgets in 2009, an investment of $89 million over six years.
CIHR has little information about the needs of health research sectors for new talent and will begin to collect information about the post-award employment of trainees who receive CIHR support. It seems likely that the majority of trainees find employment outside academia. CIHR needs to know if the students it supports have the skills sought by prospective employers.
Canada's performance in health research
Reports from individual institutes and existing CIHR publications26 provide many examples of Canadian strengths. We elected to focus here on bibliometric data that provide an overview of performance. Figures 12 to 1527 compare Canadian performance with that of the other most productive nations in the selected field. The four fields selected (medicine, neuroscience, biochemistry, genetics and molecular biology, and immunology and microbiology) represent 91% of 2008 Canadian publications28 relevant to health. In these broad fields of health research, Canadian-authored publications have increased in quantity since CIHR was established, and to a greater extent than some other established research-intensive nations.29 It should be noted that the "medicine" field includes health policy, health services, epidemiology and population health and the clinical specialities.
Canada is usually among the top four nations for citations per paper. Figures 12B to 15B show citations per publication relative to publications from the U.S. (=1).
Figure 12A: Growth in medicine publications
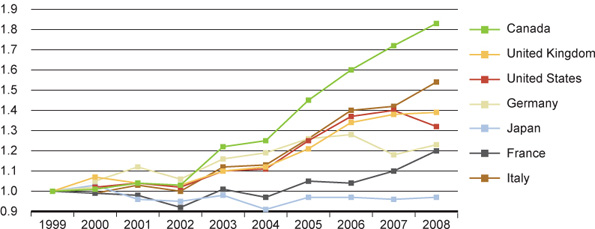
Figure 12B: Relative citations
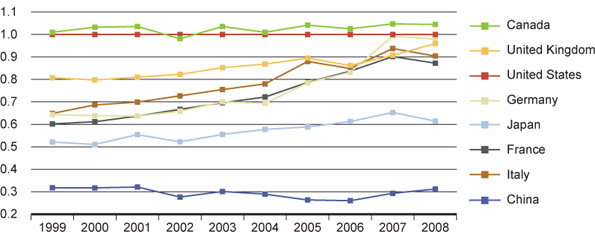
Figure 13A: Growth in neuroscience publications
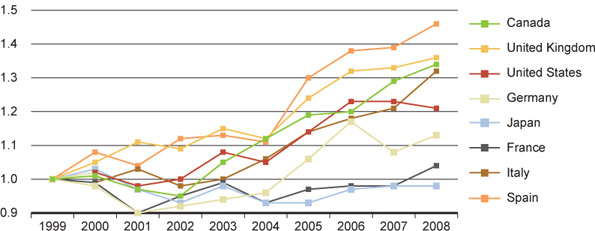
Figure 13B: Relative citations
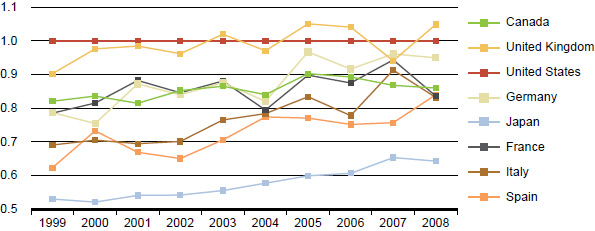
Figure 14A: Growth in biochemistry, genetics and molecular biology publications
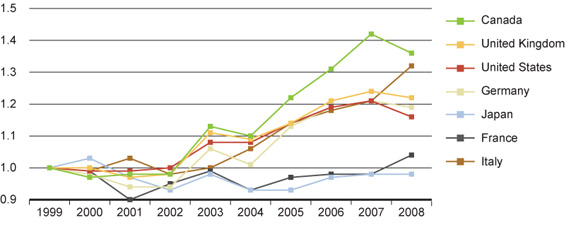
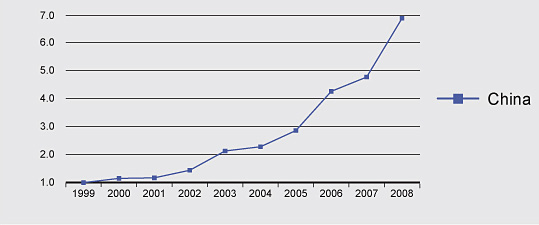
Figure 14B: Relative citations
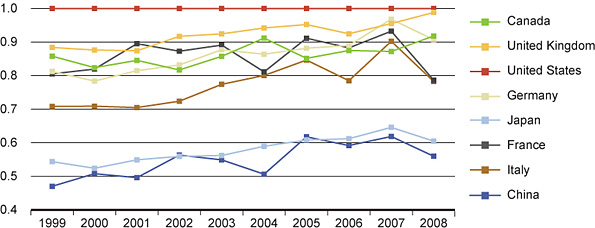
Figure 15A: Growth in immunology and microbiology publications
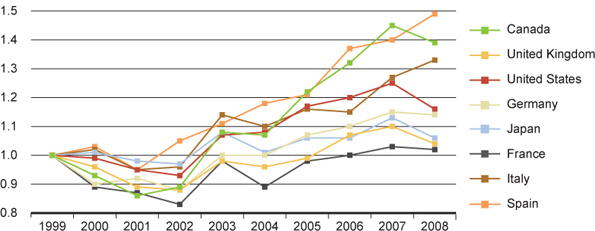
Figure 15B: Relative citations
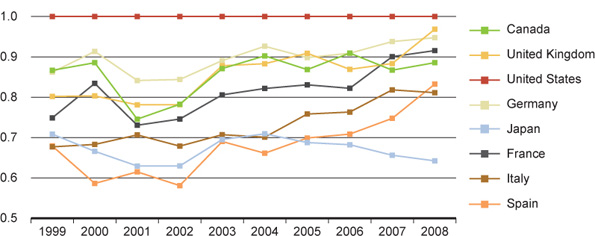
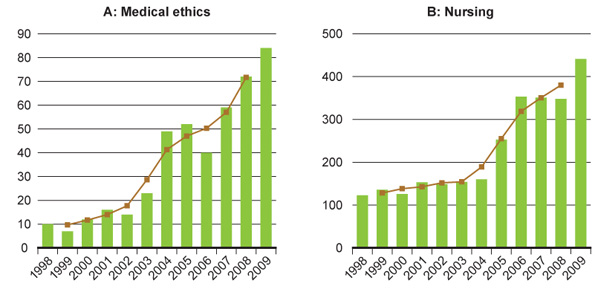
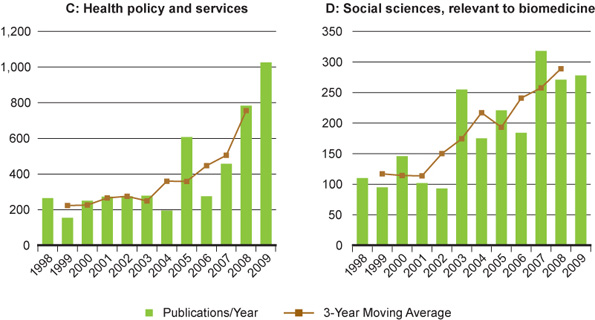
Figure 16A–D30 shows the growth in Canadian publications for more specific subfields of special relevance to the broadened mandate of CIHR, such as health ethics (eight-fold increase) and health policy and services (five-fold increase).
Another indicator of quality is the representation of Canadian authors among the most highly cited publications. With Canadian authors on 3.5% of the world's publications in medicine, we would expect to see three to four Canadian publications in the top 100 most-cited publications. However, among the 100 most-cited 1999 publications, seven have Canadian authors. Among 2006 publications, the latest year for which there is a significant citation history, 13 have Canadian authors.31 Canadian publications are also over-represented in the highest-ranked journals, with 5.3% Canadian publications in the 20 highest-impact journals in medicine for 2008. This finding is corroborated by a 2009 study32 that found Canada ranked third, behind the U.S. and Switzerland, for the proportion of health publications appearing in the top 5% of journals, as defined by impact factor. Canada ranked second in impact factor in the fields of epidemiology and preventive and occupational/environmental medicine, but much lower in public health.33 Another international comparative study34 concluded "the fact that the scientific production of researchers in Canada is higher (when adjusted for GDP) compared with other regions around the world deserves careful attention by the worldwide scientific community, as well as by public and private funding organizations, to identify the key determinants contributing to the cost-effective research productivity of this country".
Figure 16: Growth of Canadian publications in selected areas relevant to its expanded mandate
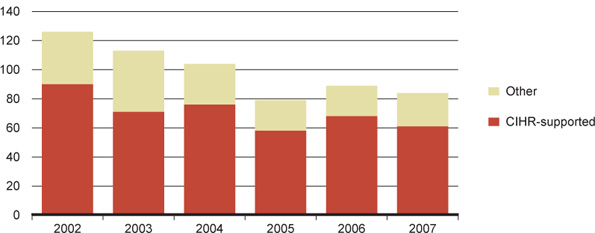
CIHR-supported research is involved in the majority of health-related U.S. patents granted to Canadian inventors35 (Figure 17).
Figure 17: U.S. patents related to health awarded to Canadian inventors
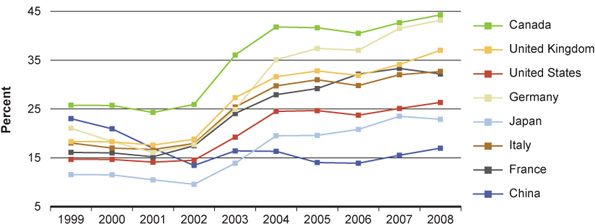
Collaboration and interdisciplinarity
The increase in international collaboration by Canadian researchers mirrors the worldwide trend, and Canadians are among the most collaborative (Figure 18 shows medicine publications only, but the same trends are evident in all other major categories). Publications co-authored with researchers from other nations have greater citation impact than purely domestic publications. For example, publications on stem cells between 2000 and 2006 that were Canadian–foreign collaborations were cited on average 44 times, while purely domestic papers were cited 29 times. In the area of health care policy and services, the citation counts over the same period averaged 16 for international collaborations and eight for domestic publications.
Consistent with the trend to increased collaboration, the average number of applicants associated with each CIHR operating grant (all programs) was 5.0 in 2009–2010, compared to 1.7 in 1999–2000. Inter-departmental and inter-institutional collaboration is common: out of a sample of 200 operating grants funded in 2009–2010, 37 involved investigators working in different departments in the same institution, and another 75 involved collaborations between investigators from different institutions. CIHR's investment in programs that specifically encourage interdisciplinary research has increased from $47 million in 2000–2001 to $112 million in 2009–2010.
Figure 18: Foreign collaboration – percentage of papers from each country with co-authors from another country
- Date modified: