Review of the Institute of Health Services and Policy Research (IHSPR)
Report of the IHSPR Review Panel
June 2018
At the Canadian Institutes of Health Research (CIHR), we know that research has the power to change lives. As Canada's health research investment agency, we collaborate with partners and researchers to support the discoveries and innovations that improve our health and strengthen our health care system.
Canadian Institutes of Health Research
160 Elgin Street, 9th Floor
Address Locator 4809A
Ottawa, Ontario K1A 0W9
This publication was produced by the Canadian Institutes of Health Research. The views expressed herein do not necessarily reflect those of the Canadian Institutes of Health Research.
IHSPR Review Panel:
Chair: Vivek Goel, Professor, Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health; Vice-President, Research and Innovation, University of Toronto
Panel Members:
- Kimberlyn McGrail, Associate Professor, Centre for Health Services and Policy Research, University of British Columbia
- Amélie Quesnel-Vallée, Associate Professor, McGill University, Joint position in the Department of Sociology and the Department of Epidemiology, Biostatistics and Occupational Health, Canada Research Chair in Policies and Health Inequalities
- Paula Rochon, Vice President, Research, Women’s College Hospital, Senior Scientist Women’s College Research Institute; Professor, Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto
- Marcel Saulnier, Associate Assistant Deputy Minister, Health Canada, Ottawa
Thanks to all participants in this review and the CIHR IHSPR Review Team: Ian Raskin, Michael Goodyer, Jean‑Christian Maillet, Kim Gaudreau, Christopher Manuel, Sheldon Polowin, Carole Chow and Doaa Saddek.
And special thanks to: Dr. Robyn Tamblyn, Scientific Director, IHSPR, Dr. Jessica Nadigel, Assistant Director, IHSPR, and the IHSPR team.
For more information and to obtain copies, please contact: Evaluation@cihr-irsc.gc.ca.
Table of Contents
- Executive Summary
- Overview of the Review
- Observations and Recommendations
- Review Key Findings
- References
- Appendices
I. Executive Summary
The review of the Institute of Health Services and Policy Research (IHSPR) was undertaken by the Canadian Institutes of Health Research (CIHR) as part of the review of the mandate and performance of CIHR Institutes by CIHR’s Governing Council (GC) outlined in the CIHR Act. The review assessed the relevance and performance of IHSPR to inform decisions regarding the role and functioning of the Institute. The review was conducted by the CIHR Evaluation Unit and overseen by a panel of experts in IHSPR’s mandate areas, the IHSPR Review Panel (hereafter referred to as the Panel), who reviewed and interpreted the findings and made the final recommendations. The observations and recommendations of the Panel are summarized below in relation to the two broad issues addressed by the review.
Are changes needed within the current IHSPR mandate in order to address emerging areas of research?
The Panel highlighted that IHSPR’s role within CIHR is unique as the Institute is responsible for: its mandate to advance health services and policy research and the application of research findings; championing the Health Systems and Services Research Theme as CIHR’s Pillar 3 Institute; and, playing a key leadership role in the development and implementation of the Strategy for Patient-Oriented Research (SPOR). There is also a close alignment between IHSPR’s and CIHR’s overall objective as it pertains to supporting and leading research that will ultimately improve the healthcare system in Canada. Given the broad and unique scope of this mandate relative to IHSPR’s defined resources, the Panel sees a need for IHSPR and CIHR to consider their respective roles and resources that could be leveraged and used collaboratively in order to facilitate stakeholder engagement and to support researchers within the health services and policy research (HSPR) community.
Recommendation 1: The Panel recommends that IHSPR continue with its current mandate.
Recommendation 2: The Panel recommends that CIHR and IHSPR clearly define their respective responsibilities and available resources to meet the interdependent needs of:
- IHSPR’s mandate;
- the Health Systems and Services Research Theme (Pillar 3); and
- CIHR’s legislated objective to excel in the creation of new knowledge and its translation into more effective health services and a strengthened Canadian health care system.
The Panel observed that the key to IHSPR’s success thus far in achieving its mandate lay in its innovative approach to capacity building. Using an embedded approach has allowed researchers and trainees to leverage their skills and expertise within the policy and decision-making space, either in health ministries or health service organizations. The Panel sees a benefit of having the next Scientific Director (SD) continue this approach and perhaps looking to expand it in a manner whereby policy and decision-makers are able to be embedded within a research setting.
Recommendation 3: The panel recommends that the Institute continue to develop innovative initiatives to build capacity in health services and policy research. In particular, the Panel suggests that working with health system partners IHSPR continue to explore mechanisms to engage those working in the health system to lead and execute research programs in partnership with the HSPR community.
Observations and Recommendations for the Next Scientific Director
The Panel noted that in order for the next SD to be successful, they will need to maintain this broad stakeholder engagement approach. Specifically, the Panel pointed to the Canadian Health Services and Policy Research Alliance (CHSPRA) and engagement with the Pan-Canadian Health Organizations (PCHOs) as two means through which the next SD is able to engage with the HSPR stakeholder community at large.
Recommendation 4: The Panel recommends that the next SD continue to engage the HSPR stakeholder community in order to both sustain and grow linkages between researchers, funding agencies, health services organizations, health charities and the 13 provincial and territorial health systems in Canada. The next SD should continue to engage with CHSPRA in developing its sustainability and closely monitor any changes in mandate or scope of the PCHOs, which could have an impact on IHSPR and the HSPR community.
The Panel considers that many elements of SPOR intersect with IHSPR’s mandate and perceives the leadership of the next SD to be critical in informing the scientific direction and leveraging the elements of SPOR that are currently entering their second phase as well as providing strong leadership on new SPOR initiatives such as the National Data Platform.
Recommendation 5: The Panel recommends that IHSPR continue the initiative it has taken to provide scientific leadership for the evolving Strategy for Patient-Oriented Research (SPOR), given the direct relevance of SPOR to IHSPR’s mandate and research and stakeholder communities.
The Panel sees it as critical that the next SD has a breadth and depth of understanding of both the research and the policy and decision-making landscapes at the federal, provincial and territorial levels as well as within health systems organizations in order to properly engage with the stakeholder community, but to also remain responsive to emerging priorities. Given the operational demands that this will likely place on the new SD, having Institute staff with a complementary set of skills will help support the new SD.
Recommendation 6: The Panel recommends that the next Scientific Director complement his/her experience and expertise with that of the Institute staff selected in light of IHSPR’s broad mandate relative to all other Insitutues and to continue to advance innovative research and ensure its translation to improve health care systems and services.
II. Overview of the Review
A. Review Objectives
The review of the Institute of Health Services and Policy Research (IHSPR) was conducted by the Canadian Institutes of Health Research (CIHR) as part of the rolling review of the mandate and performance of the 13 CIHR Institutes. The review assessed the relevance and performance of IHSPR to inform future direction and focus of its mandate. The aim of the review is to provide CIHR’s Governing Council (GC) with valid and reliable findings to inform decisions on:
- Whether changes are needed within the current IHSPR mandate to address emerging areas of research; and
- The transition of the Institute to the next Scientific Director (SD).
The review was overseen by the IHSPR Review Panel comprised of experts in the IHSPR mandate areas who reviewed and interpreted the findings and made the final recommendations. The names and affiliations of the Panel members are listed in Appendix 1. The review was conducted by the CIHR Evaluation Unit.
The review covered the period 2000-2017, with a focus on the period under the leadership of the current SD, Dr. Robyn Tamblyn, from 2011 and 2018.Footnote 1 Using a common framework of analysis, the review drew on multiple lines of evidence, including qualitative and quantitative data sources outlined in Appendix 2 with key figures presented in Appendix 3. The review used administrative data on expenditures related to the IHSPR mandate, bibliometric analysis on the ranking of Canada compared to the top active countries in the fields of health services and policy research (HSPR), interviews with a number of IHSPR researchers and stakeholder representatives and Panel deliberations. While each line of evidence has limitations, there is convergence among them so as to produce key findings. Overall, we are reasonably confident that the results presented provide an accurate portrait of the relevance of IHSPR’s mandate and the Institute’s performance.
B. CIHR Context and the Canadian Funding Landscape
As outlined in the CIHR Act, the objective of the CIHR is:
“to excel, according to internationally accepted standards of scientific excellence, in the creation of new knowledge and its translation into improved health for Canadians, more effective health services and products and a strengthened Canadian health care system…”
Among the many activities to achieve its objective, CIHR is responsible for “encouraging innovation, facilitating the commercialization of health research in Canada and promoting economic development through health research in Canada.” And, as divisions within CIHR, the Institutes are expected to contribute to the achievement of CIHR’s overall objective within their mandate through a number of activities, including: “work in collaboration with the provinces to advance health research and to promote the dissemination and application of new research knowledge to improve health and health services.” While all Institutes are to include research across all four CIHR pillars (biomedical, clinical, health systems/services and social/cultural/environmental/population health), IHSPR has a particular responsibility to promote and support pillar 3 research in health systems and health services.
In terms of funding, CIHR’s budget has been effectively flat for approximately the last 10 years, and therefore it is declining substantially in real terms, greatly affecting the ability of researchers to sustain competitive research programs. CIHR funding of research under the 13 Institutes mandate is dominated by CIHR investments in the investigator-initiated operating grant competition.Footnote 2 The Institutes’ budgets, which are used as a catalyst with strategically placed investments, are comparably smaller.Footnote 3 The final report of the Government of Canada’s Review of Federal Support for Fundamental Science, released on April 10, 2017, stressed the need for significant reinvestment in the federal research ecosystem over a more predictable and better planned multi-year horizon as well as improved coordination and collaborations between the three federal granting agencies (CIHR, NSERC and SSHRC) and the Canada Foundation for Innovation (CFI).Footnote 4 In Budget 2018, the Government of Canada made unprecedented investments in research and innovation. For CIHR, this translates to an investment of $354.7M phased in over 5 years and $90.1M ongoing in CIHR’s Investigator-Initiated research budget.Footnote 5
CIHR is composed of 13 Institutes. The original slate of Institutes was designed to ensure not only representation of all sectors and "themes" of health research, but also to provide a home base for each health researcher in Canada.Footnote 6 Each Institute received a strategic research budget of $8.6M until 2014-15. As a result of the Institute Modernization, in 2015-16, half of each Institutes’ strategic research budgets ($4.3 M per year) was invested in CIHR’s Roadmap Accelerator Fund (RAF) to support multi-Institute and multidisciplinary initiatives that aligned with CIHR’s research priorities and were patterned along the lines of existing CIHR Initiatives. The remaining half of the budget remains under the control of Institutes to direct toward Institute-specific initiatives. The RAF process was perceived by Institutes as limiting the ability of the Institutes to invest their strategic funds in Institute-specific priority areas. As of 2017-18, Institutes returned to a strategic research budget ($8.6M) and moving forward, the investments of funds in multi-Institute and multidisciplinary initiatives are guided by the same “spirit” and principles as RAF.
C. Institute of Health Services and Policy Research Context
As one of the 13 CIHR Institutes, IHSPR has a vision to position Canada as a global health leader in health services and policy research that optimizes health and health system outcomes. As part of its mission IHSPR is committed to foster excellence and innovation to catalyze the application of research findings to policies, practices and programs that provide real-world benefit and enhance the provision of high-quality care for Canadians.Footnote 7
IHSPR’s mandate is to support innovative research, capacity-building and knowledge translation initiatives designed to improve the way health care services are organized, regulated, managed, financed, paid for, used and delivered, in the interest of improving the health and quality of life of all Canadians. In addition to its role as one of CIHR’s 13 Institutes, IHSPR has the unique distinction of providing leadership for the Health System and Services theme – one of CIHR’s four pillars of health research.Footnote 8,Footnote 9 Furthermore, given its area of expertise, IHSPR staff and researchers are uniquely placed to support all of CIHR in achieving its legislated mandate of “more effective health services and products and a strengthened Canadian health care system…”.Footnote 10 Therefore, a unique challenge that IHSPR faces is the ability to engage federal and provincial partners in designing research programs that will ultimately improve the 13 provincial and territorial health systems and federal health policies and programs within Canada, while using an equity lens. Within its mandate, IHSPR establishes strategic priorities, which shape the Institute’s activities. The Institute’s current priorities are:
- The creation of learning health systems and the next generation of researchers with the skills to partner in health system learning and transformation.
- eHealth
- Healthy aging in the community
- Health system financing, funding, and sustainability.Footnote 11
III. Observations and Recommendations
A. Are changes needed within the current IHSPR mandate to address emerging areas of research?
1. Panel Observations
The Panel sees a clear and growing need for HSPR based on the high levels of spending and weak performance of healthcare systems in Canada relative to most of the Organisation for Economic Co-Operation and Development (OECD) countries.Footnote 12 The Panel highlighted that IHSPR’s role within CIHR is unique as the Institute is responsible for: its mandate to advance health services and policy research and the application of research findings; championing the Health Systems and Services Research Theme as CIHR’s Pillar 3 Institute; and, playing a key leadership role in the development and implementation of the Strategy for Patient-Oriented Research (SPOR). There is also a close alignment between IHSPR’s and CIHR’s overall objective as it pertains to supporting and leading research that will ultimately improve the healthcare system in Canada.
In order to be successful both in achieving its Institute mandate and the two additional roles that this Institute plays (as a Pillar 3 champion and SPOR leadership), the SD must also engage extensively with diverse stakeholders including the federal government, the 13 provinces and terriorities, health system organizations, and health charities. This engagement allows IHSPR to understand the various priorities of all jurisdictions in order to be responsive to their needs. These close connections to the practice, policy and research communities are essential when designing funding programs or providing scientific leadership to CIHR initiatives such as the CIHR Strategy for Patient Oriented Research (SPOR). Given the broad and unique scope of this mandate relative to IHSPR’s defined resources, the Panel sees a need for IHSPR and CIHR to consider their respective roles and resources that could be leveraged and used collaboratvely in order to facilitate stakeholder engagement and to support researchers within the HSPR community. In particular, the CIHR Executive Team should identify which of its members carries responsibilities for the legislated mandate to improve the health system and SPOR and clearly align roles and responsibilities with the IHSPR SD.
The Panel observed that the key to IHSPR’s success thus far in achieving its mandate lay in its innovative approach to capacity building. Using an embedded approach has allowed researchers and trainees to leverage their skills and expertise within the policy and decision-making space, either in health ministries or health service organizations. Conversely, many in the health system have benefited from engaging with researchers throughout the cycle from inception through dissemination, although the Panel heard that there needs to be more opportunity for those working in the health system to frame and drive the research questions. The Panel sees a benefit of having the next SD continue this approach and perhaps looking to expand it in a manner whereby policy and decision-makers are able to be embedded within a research setting. As with all federal research programs, the next SD should ensure that all the capacity building programs pay particular attention to equity and diversity at all stages of initiative design and delivery.
2. Recommendations
Recommendation 1: The panel recommends that IHSPR continue with its current mandate.
Recommendation 2: The Panel recommends that CIHR and IHSPR clearly define their respective responsibilities and available resources to meet the interdependent needs of:
- IHSPR’s mandate;
- the Health Systems and Services Research Theme (Pillar 3); and
- CIHR’s legislated objective to excel in the creation of new knowledge and its translation into more effective health services and a strengthened Canadian health care system.
Recommendation 3: The panel recommends that the Institute continue to develop innovative initiatives to build capacity in health services and policy research. In particular, the Panel suggests that working with health system partners, IHSPR continue to explore mechanisms to engage those working in the health system to lead and execute research programs in partnership with the HSPR community.
B. Observations for the Next Scientific Director
1. Panel Observations
The Panel recognizes the current SD’s unique ability to engage and be responsive to a diverse community of stakeholders, particularly in organizing workshops and meetings that allow for researchers and stakeholders from the public, private and non-profit sectors to establish crucial partnerships required for IHSPR to successfully achieve its mandate. The Panel noted that in order for the next SD to be successful, they will need to maintain this broad stakeholder engagement approach. Specifically, the Panel pointed to the Canadian Health Services and Policy Research Alliance (CHSPRA) and engagement with the Pan-Canadian Health Organizations (PCHOs) as two means through which the next SD is able to engage with the HSPR stakeholder community at large. The Panel observes that the IHSPR SD played a central role in convening CHSPRA. While the community must ultimately sustain this organization, IHSPR may need to continue to facilitate its work. The Panel also heard that the recent review of the PCHOs may result in changes in some of their mandates and configurations, and underscored the need for the HSPR community to remain engaged in their work and to facilitate their engagement with the research community.
The Panel considers that many elements of SPOR intersect with IHSPR’s mandate, and perceives the leadership of the next SD to be critical in informing the scientific direction and leveraging the elements of SPOR that are currently entering their second phase (e.g. Networks and SPOR SUPPORT Units). Further, the new SD will need to provide strong leadership on new SPOR initiatives such as the National Data Platform, which is an initative that will not only help address the access and data harmonization gaps that currently exist, but will also be instrumental in continuing to provide leadership for the development of learning health systems.
The Panel sees it as critical that the next SD has a breadth and depth of understanding of both the research and the policy and decision-making landscapes at the federal, provincial and territorial levels as well as within health systems organizations in order to properly engage with the stakeholder community, but to also remain responsive to emerging priorities. Given the operational demands that this will likely place on the new SD, having Institute staff with a complementary set of skills will help support the new SD.
2. Recommendations
Recommendation 4: The Panel recommends that the next SD continue to engage the HSPR stakeholder community in order to both sustain and grow linkages between researchers, funding agencies, health services organizations, health charities and the 13 provincial and territorial health systems in Canada. The next SD should continue to engage with CHSPRA in developing its sustainability and closely monitor any changes in mandate or scope of the PCHOs, which could have an impact on IHSPR and the HSPR community.
Recommendation 5: The Panel recommends that IHSPR continue the initiative it has taken to provide scientific leadership for the evolving Strategy for Patient-Oriented Research (SPOR), given the direct relevance of SPOR to IHSPR’s mandate and research and stakeholder communities.
Recommendation 6: The Panel recommends that the next Scientific Director complement his/her experience and expertise with that of the Institute staff selected in light of IHSPR’s broad mandate relative to all other Insitutues and to continue to advance innovative research and ensure its translation to improve health care systems and services.
IV. Review Key Findings
A. Relevance
1. Ongoing relevance of the IHSPR mandate
Prior to the creation of CIHR in 2000 and the establishment of IHSPR, there was limited capacity for health services and policy research in Canada, with only a few relatively small funders including the National Health Research Development ProgramFootnote 13 and the Canadian Health Services Research Foundation (CHSRF).Footnote 14 Since its creation and through its first decade, IHSPR has moved rapidly with programs designed to build capacity, identify evidence gaps and emerging health system challenges, support innovative research, engage decision makers and foster timely knowledge translation, and work closely with all CIHR Institutes to integrate health services and policy research within all strategic funding programs and initiatives.Footnote 15
In March 2018, the final report of the External Review of the Pan-Canadian Health Organizations (PCHO) was released. It provides advice and recommendations to the Minister of Health on how to improve the current PCHO suite. A direct quote from the report indicates the need for more funding in health services and policy research. “We heard from many health sector stakeholders about the need for a significant expansion of practical, applied, policy-focused or “policy-ready” research in Canada. The research programs operated by CHSRF in its early years helped support this type of research, and there was an expectation that additional support would flow from CIHR and its Institute of Health Services and Policy Research when those programs were transferred from CHSRF. However, only a small portion of CIHR’s budget (eight per cent) is dedicated to health services and policy research, with limited focus on evaluation and other applied policy issues. There is an opportunity for the PCHOs to work with CIHR (and perhaps Health Canada more broadly) to explore the potential for synergies in improving support for applied policy research”.Footnote 16
From 2000-01 to 2016-17, the average annual investment in IHSPR’s mandate represented 10% of CIHR’s total expenditures and, for 2016-17, CIHR’s investment in IHPSR’s mandate ranked 8th among the 13 Institutes. Interestingly, the largest percentage of total CIHR investment in IHSPR’s mandate research area has been through priority-driven research funding opportunities rather than investigator-initiated research, despite the partitioning of CIHR’s core funding budget in favour of investigator-initiated research over priority driven research. For more information about CIHR investments in IHSPR’s mandate by research priorities, see Appendix 3.
IHSPR has an annual Institute-Specific Initiative (ISI) budget, which returned to $8.6M in 2017-18, and is used to invest in a wide variety of research activities to address areas of strategic importance. IHSPR has taken a “relevance by design” approach to develop its strategic directions and guide its investments in novel program development and funding opportunity design to build linkages between researchers and decision makers, while ensuring relevance to health system needs.
The IHSPR 2015-2019 Strategic Plan focuses on four research priorities:
- The Creation of Learning Health Systems and the Next Generation of Researchers with the Skills to Partner in Health System Learning and Transformation
- eHealth
- Healthy Aging in the Community
- Health System Financing, Funding, and Sustainability
From 2014-15 to 2016-17, CIHR invested across all four of these priorities with Health System Funding, Financing and Sustainability receiving on average $21M during this period. The remaining three research priorities all gradually received more CIHR funding during the same period, most notably, expenditures for Learning Health Systems increased from $11.5M to 19.7M.
IHSPR investment in CIHR Initiatives out of its own budget increased from 11% in 2011-12 to 56% in 2014-15. Over the period from 2011-12 to 2016-17, IHSPR contributed financially to eight out of CIHR’s 27 current major initiativesFootnote 17. These are Community-Based Primary Health Care (CBPHC), eHealth Innovations, Evidence-Informed Health Care Renewal (EIHR), Personalized Medicine, Personalized Health, SPOR, Pathways for Health Equity for Aboriginal Peoples, and the Drug Safety and Effectiveness Network (DSEN). The highest contribution was in CBPHC, which accounted for 28% of IHSPR’s budget over this 6-year period.
The bibliometric analysisFootnote 18 shows that between 2000 and 2016, Canada ranks 3rd among top 10 most productive nations in number of publicationsFootnote 19 in all five HSPR priority areasFootnote 20 combined, with Canadian researchers publishing in journals that are cited more often than the world average. During the same period, the Specialization Index (SI)Footnote 21 shows that Canada is more specialized across the five priority areas as whole, compared to the world average. In fact, Canada ranks 3rd amongst the top 10 most productive countries for the SI of publications. These results are consistent with the findings from the recent report from the Canadian Council of the Academies report: Competing in a Global Innovation Economy: Current State of R&D in Canada. The bibliometric analysis conducted in this report found that when measured on a composite scale that includes measures of magnitude, impact and growth, Public Health and Health Services Research in Canada ranked 4th in research strength among Canada’s top 20 disciplines. Of note, clinical medicine was ranked 3rd and biomedical research 14th. In its subfield analysis, two IHSPR areas, Medical Informatics and Health Policy and Services were 6th and 8th in the country with General and Internal Medicine at 2nd and Rehabilitation at 10th (both of which include significant HSPR). Furthermore, the combined Public Health and Health Services Research category was one of the few Canadian areas of research to show growth from the previous CCA analysis.
All lines of evidence indicate that IHSPR has engaged the broader HSPR community, in designing a program of research intended to meet its mandate. The IHSPR stakeholders interviewed generally agree that IHSPR has managed to meet its mandate, especially considering the broadness of the mandate and the limited funds available. They also recognized the current SD’s effort to align IHSPR’s research priorities to those of the 13 different health systems in Canada. Specifically, interviewees cited the Health System Impact Fellowships, Embedded Clinician Scientist and the SPOR: Rewarding Success Initiative as examples of initiatives designed to specifically to meet health systems needs.
B. Impact
1. Support to Innovative Research and Advancing Knowledge
IHSPR, under the direction of the current SD, has continued its efforts to emphasize capacity building by making it one of its strategic priorities in its latest strategic plan. IHSPR has developed innovative approaches to capacity building through initiatives like the Health Systems Impact Fellowships and Embedded Clinician-Scientists, and through the organization of several workshops and annual meetings that allow for HSPR researchers to come together with other stakeholders in the HSPR community thereby creating a forum for research collaborations and knowledge exchange.
IHSPR’s “relevance by design” approach to initiative development and their innovative approach in capacity building would not have been successful without the current SD’s commitment to engaging the broad HSPR stakeholder community. This IHSPR-led process resulted in the launch of the Canadian Health Services Policy Research Alliance (CHSPRA), which includes more than 41 federal and provincial research funders, health charities, health systems organizations, and university HSPR training programs.
Given the close proximity of HSPR to the health system, it is not surprising that this type of research can have a direct impact on health systems in minimal time. In an effort to gauge the influence of HSPR research on health systems, CIHR collected and identified all relevant IHSPR mandate related ‘knowledge products’ (KP) that were supported by CIHR funding and ran a matching process with the Observable Influence Beyond Academia (OIBA) database, which is maintained by CIHR’s Results and Impact Unit. The analysis of the KPs revealed that the percent matching of IHSPR mandate-related KPs to the OIBA database more than doubled the CIHR supported KPs as a whole (Appendix 3)
Through IHSPR’s innovative approach to designing funding opportunities, the Institute has been able to maximize the impact of its limited strategic budget by funding smaller grants that have a large impact on the health system. One such example is the work of Dr. Shelley Doucet at the University of New Brunswick. As a recipient of and IHSPR funded operating grant, Dr. Doucet and her team were able to identify gaps and barriers to care for children with complex health conditions, leading to the development of a new service delivery model: NaviCare/SoinsNavi. The findings from this study led to a Best Brains Exchange in February 2018 and are being used to inform potential scale up and adoption of this service model in Prince Edward Island.
As part of CIHR’s Community-based Primary Health Care (CBPHC) Initiative, which is co-led by IHSPR, the Living with HIV (LHIV) CBPHC Innovation Team, funded by IHSPR and led by Drs. Liddy and Kendall, has taken the BASE eConsult Program, developed by Dr. Liddy, and tested, implemented and scaled it up. The program allows primary care providers to connect patients to specialists through e-consultation and has supported speedier access – an average of 2 days response time. Between 2011 and 2015 over 10,000 eConsults led to only 29% needing a face-to-face referral. Instead, many unnecessary face-to-face specialist visits were prevented and deemed not necessary as a result of the eConsult service. Dr Liddy’s team demonstrated cost savings, $42.42/consultation versus $133.60/visit for traditional face-to-face consultation visits. The program was initially implemented in one health region of Ontario and has now been spread to other regions in Ontario. The team is now working to expand the eConsult service to Manitoba and Newfoundland and Labrador.
Some of the researchers and stakeholders interviewed commended the SD and IHSPR for understanding the research-practical issue linkages inherent to HSPR research, which has helped bringing knowledge translation to the forefront in IHSPR’s initiatives. IHSPR-funded projects in the area of primary healthcare and SPOR were often cited as examples.
2. Contributions to Building Capacity of the Health Research Enterprise
All lines of evidence demonstrate that capacity building is one of IHSPR’s greatest strengths. From 2001 to 2016, IHSPR’s investments in capacity building accounted on average for 40% of its budget. These include investments in catalyst/pilot programs; training grants and awards; and development grants (see Appendix 3). As of 2016-17, 10% of total CIHR funded direct traineesFootnote 22 and 14% of indirect traineesFootnote 23 were funded under IHSPR’s mandate (see Appendix 3).
An overarching approach to IHSPR’s capacity building strategy has been to enable health system innovation by embedding researchers and trainees in the health system. Through initiatives such as the Embedded Clinician Researcher Salary Awards, and the Training Modernization in Health Services and Policy Research Initiative, the health system is able to leverage the skills of researchers to help work on health system priorities. Likewise, this capacity building model allows for the training the next generation of health systems researchers that will be able to partner with clinical and policy leaders to identify priorities and be responsive to health systems needs.
IHSPR convenes a number of meetings on an annual basis such as the Health System Impact Fellowship National Cohort Meeting and the CBPHC Annual Meeting. These capacity building events provide trainees, researchers and key HSPR stakeholders and partners opportunities to establish collaborations, participate in knowledge exchanges and form partnerships between researchers and other members of the broader health systems community. In addition, IHSPR has developed several funding programs under the Institute Community Support (ICS)Footnote 24 Program to encourage excellence in research and foster community development.
All stakeholders interviewed expressed strong support for IHSPR’s approach to capacity building. Interviewees from the research community, health system organizations and provincial governments spoke favorably of the benefits of having researchers and trainees embedded in the health system. One early career investigator attributed IHSPR’s capacity building efforts to their success in CIHR’s Project Grant Competition. All interviewees believed that IHSPR’s capacity building effort under the Learning Health Systems strategic priority should continue under the leadership of the next SD.
C. Convener and Catalyst
1. Contribution of Scientific Leadership to the Convener-Catalyst Role
IHPSR has used a variety of networking and stakeholder engagement approaches to help bring together various health services and policy stakeholders together, ranging from creating stakeholder alliances and international partnership opportunities, to hosting meetings and symposia as part of IHSPR-led strategic initiatives.
Many stakeholders interviewed cited CHSPRA as an example of the SD’s leadership in her convener and catalyst role. CHSPRA was born out of an IHSPR-led process that began in 2013 to bring together key stakeholders in health services and policy research. This process involved the creation of an asset map and preliminary strategic analysis, which culminated into the first ever pan-Canadian vision and strategy for HSPR, which was published in 2015. Over time, the initial group of 25 stakeholders grew to include more than 41 federal and provincial research funders, health charities, health system organizations and university HSPR training programs. CHSPRA has identified three priorities, and working groups have been struck to advance work on each priority: Training Modernization Working Group, Impact Analysis Working Group, and Learning Health Systems Working Group
In recent years, IHSPR has formed international partnerships, particularly with the European Union. Initiatives such as TO-REACH,Footnote 25 Active and Assisted Living (AAL), More Years Better Lives, and ITEA, provide Canadian health services and policy researchers, and their partners, to establish international collaborations for joint learning opportunities and establish a critical mass to advance the knowledge base in HSPR. A particularly innovative approach in the HSPR area was the partnership with the National Research Council’s Industrial Research Assistance Program (NRC IRAP) to bring start-ups and small and medium enterprise companies together with health system stakeholders and researchers.
The majority of stakeholders interviewed stressed how crucial partnership development across multiple stakeholder groups including but not limited to provincial and territorial ministries of health; health system organizations; and private sector is for IHSPR to set research priorities that are responsive to health system needs and ultimately be successful in meeting its mandate. They also observed that the current SD has been responsive and successful in fostering partnerships, which was particularly beneficial to the research community, particularly early career researchers, who may not have been able to make these connections on their own. Some stakeholders view an opportunity for IHSPR and CIHR to collaborate with the Pan-Canadian Health Organizations in setting common priorities for health system improvement.
2. Partnering to Achieve CIHR and Institute Objectives
IHSPR partnerships and collaborations with other entities took several forms, such as collaborating and convening to enable knowledge exchange and networks of researchers and practitioners, raising more research funding as well as increasing the capacity within specific areas. Partner organizations include all the other CIHR Institutes, government agencies and departments, international partners and not-for-profit organizations, such as health charities (see Appendix 4).
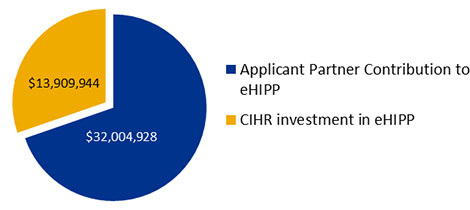
IHSPR has been very successful at leveraging partner contributions, at both a competition and applicant level, to funding opportunities funded from their own budget. This is due in part to the mandatory partnership requirements on many IHSPR-associated funding opportunities. The leverage ratio over IHSPR’s 16-year period is 0.28, which means for every $100 invested out of IHSPR’s budget there is $28 leverage from external partners. However, due to limitations on how CIHR tracks applicant partners, this only partially reveals IHSPR’s success. For example, in the eHealth Innovations Partnership Program (eHIPP) Operating Grant competition, applicants were required to secure partnership contributions as a prerequisite to apply. An examination of the applicant partnership data reveals that applicant partner contributions accounted for 70% of the investment in the eHIPP operating grant funding opportunity, whereas CIHR’s investment accounted for the remaining 30%, which translates to a leverage ratio of 2.3 for this particular funding opportunity. (See Appendix 3).
D. Operational Effectiveness
The Institution within which IHSPR operates receives $1 M annually from CIHR as an Institute Support Grant (ISG). Before 2011-12, IHSPR did not spend all of its ISG funding annually, the balance was transferred to the following fiscal year and therefore the total annual funds available for ISG exceed the $1M allotment to the Institute every year (see Appendix 3). Between 2011-12 and 2016-17, IHSPR spent an annual average of 67% on Institute Operations (which include staff salary) and the remainder was used for Institute Strategic Development (ISD). IHSPR uses the ISD portion of its budget to support convener and catalyst and capacity building activities such as Institute Advisory Board meetings, workshops and annual meetings.
CIHR’s structure and approach to the staff allocated to support the 13 institutes has changed in recent years. Before 2014-15, there were Ottawa-based Institute staff (OBIS) at CIHR’s central office, each of whom was dedicated to provide service to each of the 13 Institutes. After that, the staff allocation model changed to Institute based staff, working in Integrated Institute Teams (IIT) that provide support across all 13 Institutes. This change is seen to have undermined the ability of building corporate memory, continuity and staff loyalty within an Institute, as well as creating pressure on the Institute operating budget to cover staffing costs that were previously covered by CIHR’s central office.
A possible approach to address IHSPR’s broad mandate, key roles within CIHR, and the loss of a dedicated Ottawa-based Instititue Assistant Director, the next IHSPR SD should consider hiring an additional Assistant Director to facilitate the broad stakeholder engagement that is required; specifically, in relation to IHSPR’s Pillar 3 and SPOR leadership roles.
V. References
- Government of Canada, Budget 2018 – Equality + Growth: a Strong Middle Class, 2018
- Investing in Canada’s Future: Strengthening the Foundations of Canadian Research. Canada’s Fundamental Science Review (2017)
- CIHR, IHSPR, Strategic Plan 2015-2019
- Fit for Purpose: Findings and Recommendations of the External Review of the Pan-Canadian Health Organizations
- Competing in a Global Innovation Economy: The Current State of R&D in Canada [ PDF (6 MB) - external link ]
- Overview of the Reforms to CIHR’s Open Suite of Programs: Peer Review Expert Panel
VI. Appendices
Appendix 1: IHSPR Review Panel Members’ Affiliations and Conflict of Interest Declaration
Chair:
- Vivek Goel, Vice-President, Research and Innovation, University of Toronto; Professor, Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto
Panel Members:
- Kimberlyn McGrail, Associate Professor, University of British Columbia
- Amélie Quesnel-Vallée, Associate Professor, McGill University, Joint position in the Department of Sociology and the Department of Epidemiology, Biostatistics and Occupational Health, Canada Research Chair in Policies and Health Inequalities
- Paula Rochon, Vice President, Research, Women’s College Hospital, Senior Scientist Women’s College Research Institute; Professor, Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto
- Marcel Saulnier, Associate Assistant Deputy Minister, Health Canada, Ottawa
| Panel Member | Conflict of Interest Declaration |
|---|---|
| Vivek Goel | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Evaluation Panel |
| Kimberlyn McGrail | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Evaluation Panel |
| Amélie Quesnel-Vallée | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Evaluation Panel |
| Paula Rochon | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Evaluation Panel |
| Marcel Saulnier | Confirmed no real, apparent or potential conflict(s) of interest with respect to his involvement with the Evaluation Panel |
Appendix 2: Overview of Data Sources and Methods
| Data source | Description |
|---|---|
| Situational Analysis (SA) |
|
| Key informant interviews |
|
| Bibliometric Analysis |
|
Appendix 3: Key Figures and Tables
- Figure A: CIHR Investment in IHSPR Mandate by 2014-15 to 2016-17 Research Priorities
- Figure B: Investment in Capacity Building out of IHSPR Budget
- Figure C: Percentage of Direct Trainees Funded under IHSPR Mandate
- Figure D: Percentage of Indirect Trainees Supported under IHSPR Mandate
- Figure E: IHSPR Mandate-Related CIHR Supported Observable Impact Beyond Academia Data
- Figure F: Partner Contributions to IHSPR Funding
- Figure G: Utilization of Institute Support Grant (ISG) Budget
Figure A: CIHR Investment in IHSPR Mandate by 2014-15 to 2016-17 Research Priorities
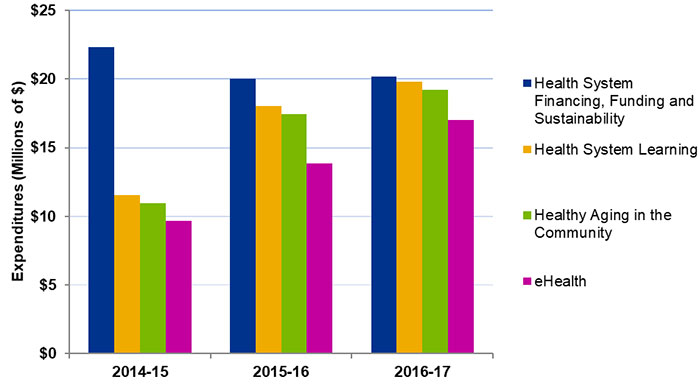
Figure A – Long description
| 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|
| Health System Financing, Funding and Sustainability | $22,304,110 | $20,006,804 | $20,192,963 |
| Health System Learning | $11,547,460 | $18,052,660 | $19,793,123 |
| Healthy Aging in the Community | $10,973,872 | $17,430,813 | $19,224,975 |
| eHealth | $9,677,838 | $13,827,593 | $16,994,539 |
Figure B: Investment in Capacity Building out of IHSPR Budget
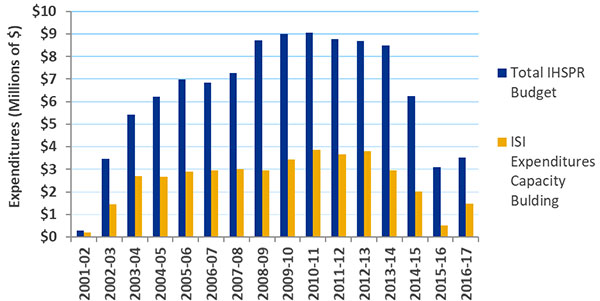
Figure B – Long description
| 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total IHSPR Budget | 290,464 | 3,458,650 | 5,430,055 | 6,222,914 | 6,970,980 | 6,836,898 | 7,270,652 | 8,723,174 | 8,995,900 | 9,054,340 | 8,777,587 | 8,682,980 | 8,472,956 | 6,236,743 | 3,081,171 | 3,522,684 |
| ISI Expenditures Capacity Building | $191,345 | $1,443,311 | $2,705,634 | $2,676,167 | $2,903,169 | $2,966,919 | $3,022,192 | $2,960,943 | $3,446,987 | $3,873,290 | $3,671,302 | $3,813,800 | $2,944,016 | $2,018,493 | $505,848 | 1,486,596 |
Figure C: Percentage of Direct Trainees Funded under IHSPR Mandate
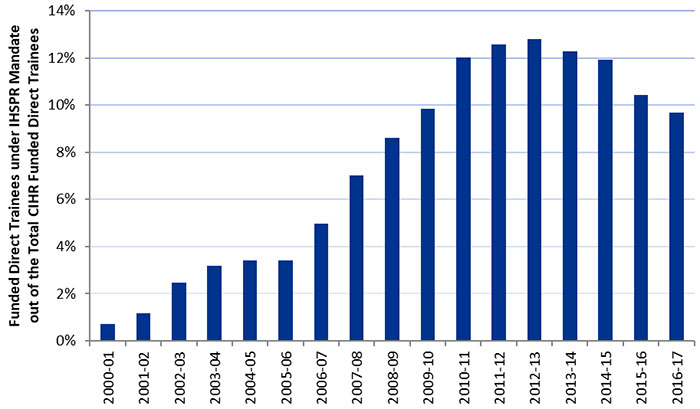
Figure C – Long description
| 2000-01 | 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % of Funded Direct Trainees under IHSPR Mandate out of the Total CIHR Funded Direct Trainees | 1% | 1% | 2% | 3% | 3% | 3% | 5% | 7% | 9% | 10% | 12% | 13% | 13% | 12% | 12% | 10% | 10% |
Figure D: Percentage of Indirect Trainees Supported under IHSPR Mandate
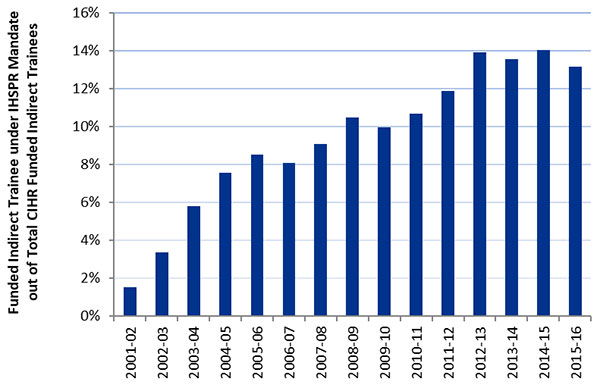
Figure D – Long description
| 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % of Funded Indirect Trainees under IHSPR Mandate of Total CIHR Funded Indirect Trainees | 2% | 3% | 6% | 8% | 9% | 8% | 9% | 10% | 10% | 11% | 12% | 14% | 14% | 14% | 13% |
Figure E: IHSPR Mandate-Related CIHR Supported Observable Impact Beyond Academia Data
| Indicator | IHSPR | CIHR | ||
|---|---|---|---|---|
| 2008-2016 KP PYs | 2008-2010 KP PYs* | 2008-2016 KP PYs | 2008-2010 KP PYs* | |
| # of CIHR supported KPs | 2,625 | 505 | 69,510 | 16,267 |
| % of KPs with OIBA | 19.9% (n=523)** | 38% (n=192)** | 8.2% (n=5,719)** | 18.3% (2,984)** |
| % of KPs with OIBA on Downstream Documents | 19.8% (n=519) | 37.2% (n=188) | 6.2% (n=4,290) | 9.6% (n=1,555) |
| % of KPs with OIBA on Patents | 0.3% (n=7)*** | 1.4% (n=7)*** | 2.1% (n=1,493)*** | 9.2% (n=1,493)*** |
|
||||
Figure F: Partner Contributions to IHSPR Funding
Leverage Ratio of Partnership to CIHR Investment in IHSPR Mandate
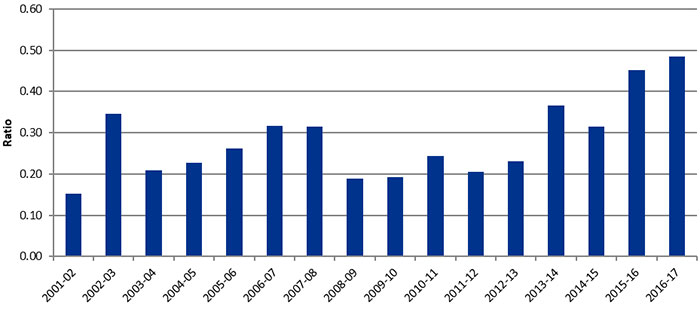
Figure F – Long description
| 2001-02 | 2002-03 | 2003-04 | 2004-05 | 2005-06 | 2006-07 | 2007-08 | 2008-09 | 2009-10 | 2010-11 | 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Leverage Ratio | 0.15 | 0.35 | 0.21 | 0.23 | 0.26 | 0.32 | 0.31 | 0.19 | 0.19 | 0.24 | 0.20 | 0.23 | 0.37 | 0.32 | 0.45 | 0.49 |
- The leverage ratio of partnership to IHSPR investment shows how much was invested in the IHSPR’s mandate area through partner contributions, for every dollar invested out of IHSPR’s budget in the mandate areas.
Applicant Partner Contribution to eHIPP Operating Grant Funding Opportunity
Applicant Partner Contribution to eHIPP Operating Grant Funding Opportunity – Long description
| Applicant Partner Contribution to eHIPP | $32,004,928 |
|---|---|
| CIHR investment in eHIPP | $13,909,944 |
Figure G: Utilization of Institute Support Grant (ISG) Budget
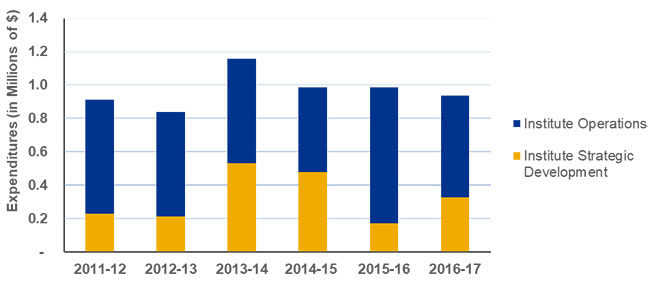
Figure G – Long description
| 2011-12 | 2012-13 | 2013-14 | 2014-15 | 2015-16 | 2016-17 | |
|---|---|---|---|---|---|---|
| Institute Strategic Development | $227,991 | $211,252 | $531,531 | $477,450 | $170,101 | $327,526 |
| Institute Operations | $685,019 | $625,348 | $627,516 | $508,634 | $813,629 | $608,874 |
| Total expenditures | $913,010 | $836,600 | $1,159,047 | $986,084 | $983,730 | $936,400 |
Appendix 4: Sample list of Partners
- Michael Smith Foundation for Health Research
- Fonds de recherche santé du Québec
- Alberta Innovates
- NewBrunswick Health Research Foundation
- Saskatchewan Health Research Foundation
- Research Manitoba
- Newfoundland Centre for Applied Health Research
- Province of Ontario
- Nova Scotia Health Research Foundation
- Canadian Association for Health Services and Policy Research
- EvidenceNetwork.ca
- Universitatea Babes-Bolyai
- The College of Family Physicians of Canada
- Inserm
- Forte:
- State of Israel Ministery of Health
- AGE-WELL
- Health Research Council of New Zealand
- Health Research Board
- Mc Master Health Forum
- Public Health Agency (Northern Ireland)
- Australian Primary Health Care Research Institute
- Suomen Akatemia
- North American Primary Care Research Group
- Canadian Patient Safety Institute
- ZonMw
- European Health Management Association
- Forskningsradet
- Robert Graham Center
- University of Malta
- Agency for Healthcare Research and Quality
- Gesundheit Österreich
- European Public Health Association
- McConnell Foundation
- Date modified: