Partnerships for Better Health – CIHR-ICRH Strategic Plan 2022-2025
The Challenge
- The Challenge
- A Framework for Decision-Making
- A Unifying Approach
- Priority A: Preparing Future Capacity
- Priority B: Accelerating Knowledge Through Collaboration
- Priority C: Catalyzing Impact Through Knowledge Mobilization
- Theme 1: Strengthening Indigenous Health Research
- Theme 2: Enhancing Equity, Diversity and Inclusion in Health Research
- Strategic Plan in Action
-
Land Acknowledgment
We respectfully acknowledge that the land on which we developed The Plan is Treaty 6 Territory in Western Canada, the traditional meeting ground and home for many First Nations Peoples (Cree, Saulteaux, Niisitapi [Blackfoot], and Nakota Sioux) and Métis Peoples. We acknowledge their diverse histories and cultures, and we pay respect to all Indigenous Peoples (First Nations, Inuit, and Métis), from coast to coast to coast, for their past and ongoing contributions to society. We strive for respectful partnerships with Indigenous Peoples as we search for healing and true reconciliation.
-
Message from the Scientific Director

It gives me great pleasure to introduce you to the 2022–2025 CIHR Institute of Circulatory and Respiratory Health (ICRH) Strategic Plan (The Plan).
The Plan follows our 2017–2020 Refreshed Strategic Plan, which focused on capacity development, networking and equity, diversity and inclusion (EDI) in health research. Much has changed since those early days of my first term as Scientific Director. First, the development and release of The Plan was interrupted by the Severe Acute Respiratory Distress Syndrome coronavirus-2 (SARS-CoV-2 or COVID-19) pandemic. Second, CIHR released an organizational Strategic Plan designed to encompass the period from 2021-2031. Finally, the commitment to EDI and Indigenous health research (IHR) has increased, at ICRH, within CIHR and across the entire Canadian health research ecosystem. The only thing that is consistent appears to be change itself.
The COVID-19 pandemic is an unprecedented global health crisis that has affected everyone around the world. To the relief of many, knowledge creation and translation as well as iterative policy changes based on emerging research evidence have been at the forefront of the crisis. From the use of masks and physical distancing to the evaluation of acute COVID-19 treatments in platform trials and the development, trialing and uptake of vaccines, science has driven much of the decision-making throughout the pandemic. Unfortunately, misinformation, social media and political divisions have resulted in vaccine hesitancy and anti-vaccination posturing. Consequently, CIHR has funded research to understand misinformation and implement policies and interventions to maximize vaccine uptake.
The pandemic has also been an innovation accelerator. Some of the innovations have been long overdue, some have had unintended consequences and some represent permanent solutions. For example, prior to the pandemic virtual meetings, working from home and virtual care practices were uncommon; however, not a day goes by now without virtual interactions. Collaboration, data-sharing and rapid research responses have been the keys to addressing the pandemic and advancing science.
In collaboration with our leadership and staff at the CIHR Capital Region, the ICRH staff have worked diligently during the pandemic to contribute to the CIHR medical countermeasures funding opportunities, the Centre for Research on Pandemic Preparedness and Health Emergencies, the Clinical Trial Fund and strategic funding within the Institute mandate areas (e.g., Transitions in Care, Sepsis Research Network, Heart Failure Research Network and the Sleep Research Consortium). We have remained in regular contact with partnership groups such as the Health Charities Coalition of Canada, the National Heart, Lung and Blood Institute at the National Institutes of Health and many more external Institute partners (e.g., charities, societies, industry, and other partner groups). These interactions have reemphasized the importance of every partner within the health research ecosystem resulting in the central tenet of The Plan: Partnerships. Clearly, the critical contributions of science during the pandemic have illustrated the power of collaboration with partners.
During the extensive consultation process for this new strategic plan, we have heard from people with lived experience (PWLE), scientists, funders and other partners. Rather than simply developing a short- and medium-term recovery plan, our partners challenged us to produce a plan focused on creating an environment that will permit the ecosystem to recover and improve. In that vein (pun intended), we are proposing a bold model focused on partnerships: with other Institutes, within CIHR and with external partners. We recognize the challenges partners have experienced during the pandemic; however, the pandemic has reconfirmed the critical role the various partners play in the stability of the health research ecosystem. Their resilience and collaboration have been an inspiration to both the Institute team and me.
The Plan represents the culmination of many months of dialogue and listening with our community. We have focused on three strategic priorities: Preparing Future Capacity, Accelerating Knowledge Through Collaboration and Catalyzing Impact Through Knowledge Mobilization. In addition, Strengthening IHR and Enhancing EDI in Health Research reflect two foundational themes that the Institute has focused on over the past six years and will continue to champion in the future.
We believe the strategy is comprehensive and nimble. Most importantly, given the difficulty of gazing into the crystal ball and predicting the future, the strategy is disease and health research topic agnostic. For example, regardless of the health research issue we apply the strategy to (e.g., artificial intelligence, mandate-specific health conditions, climate change, clinical trials, pandemic preparedness and health emergencies, prevention, etc.), the three strategic priorities and the two foundational themes will resonate with partners in the research community. Together, we are excited to apply our Plan to the health challenges you believe are important to your community!
In closing, I am indebted to all of the members of the Institute Advisory Board (IAB), led by Dr. PJ Devereaux (Chair) and Dr. Marilyn MacKay-Lyons (Vice-Chair), who have provided so much of their time and expertise to advance the strategic planning for the Institute. I also want to acknowledge all of the participants from the community who helped shape the Plan, and the MP Strategies Group (MPSG) for their assistance in coordinating the engagements and writing. Finally, it is essential for me to acknowledge the efforts of the team at ICRH, including Dr. Ryan Perry, Dr. Helen Coe, Ebele Unaegbunam and Kaylin Barnes, for their hard work, commitment, and flexibility through this very challenging period. Working with the IAB, our dedicated ICRH team and the MPSG consultants on the Plan has been a highlight for me.
We are building Partnerships for Better Health and our team looks forward to engaging with our incredible research community to advance the generation and implementation of science in our mandate areas.
Sincerely,
Brian H. Rowe, MD, MSc, CCFP(EM), FCFP, FCCP, FCAHS
Scientific Director, Institute of Circulatory and Respiratory Health
Canadian Institutes of Health ResearchProfessor, Department of Emergency Medicine,
Faculty of Medicine & DentistryProfessor, School of Public Health
College of Health Sciences, University of Alberta -
Executive Summary
The Institute of Circulatory and Respiratory Health (ICRH) mandate areas represent some of the most important health conditions affecting Canadians and people across the globe.
These circulatory (e.g., cardiovascular, brain [stroke], critical care, blood and blood vessels) and respiratory (e.g., lung and sleep) conditions within ICRH account for the highest number of deaths, hospitalizations, need for critical care, emergency department visits and comorbid conditions in Canada. Investment in these areas is critically important to the health and wellness of Canadians.
The ICRH Strategic Plan (The Plan) is designed to guide the Institute through the next four years (2022–2025), the transition to the next Scientific Director (starting in January 2024) and a period of recovery and growth following the pandemic.
The Plan represents the culmination of many months of dialogue and listening to our community with the aim to advance Canada’s position as a leader in addressing circulatory and respiratory health and wellness challenges for all people living in Canada. The Plan is informed by a decision-making framework and includes the following:
A Central Tenet
- Partnerships: To enhance existing and build new partnerships with other Institutes, within CIHR and with external partners, including people with lived and/or living experience.
Three Strategic Priorities
- Preparing Future Capacity: To attract, retain and develop future research and knowledge leaders within the Institute mandate areas;
- Accelerating Knowledge Through Collaboration: To create and support innovative purpose-driven research collaborations to generate knowledge within the Institute mandate areas; and,
- Catalyzing Impact Through Knowledge Mobilization (KM): To maximize the application and impact of new and existing knowledge created by and for the ICRH research community.
Two Foundational Themes
- Strengthening Indigenous Health Research (IHR): To champion the conduct of research led by Indigenous Peoples and people with demonstrated culturally safe engagement with Indigenous communities; and,
- Enhancing Equity, Diversity and Inclusion (EDI) in Health Research: To support ICRH mandate area activities that are conducted on and/or by those who represent the diversity and intersectionality of ICRH community members and stakeholders.
The Plan in action is exemplified in the following Institute strategic activities:
- Heart Failure (HF) Research Network ($5M investment over 5 years) – To strengthen IHR in areas of need, the Institute includes Indigenous-led requirements within many of its strategic funding opportunities such as the HF Research Network.
- Sleep Research Consortium ($5M investment over 5 years) – Funding sleep research using a consortium model enabled the support of individual research teams that focused on specific research areas relevant to sleep hygiene and insomnia while at the same time providing a framework for coordination of key cross-cutting activities among the research teams.
- Transitions in Care (TiC) Initiative ($35M investment starting in 2017) – The TiC Initiative was developed through strategic partnerships that supported several funding components that addressed knowledge gaps, identified evidenced-based practices and supported the embedding of health system-decision makers within implementation science teams to address care transition challenges.
- Health Research Training Platforms (HRTPs) (total CIHR investment of $31.1M over 6 years) – The HRTPs are designed to ensure that health research trainees and early career researchers are best positioned to navigate a dynamic health research landscape with evolving research directions, practices and technologies.
The Plan guides the Institute through a period of recovery and growth following the pandemic and by listening and working with our stakeholders, we aim to achieve Partnerships for Better Health.
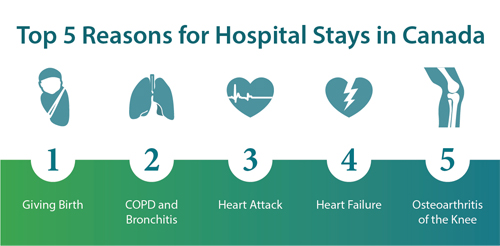
Top Five Reasons for Hospital Stays in Canada
Long description
Reason 1 – Giving Birth
Reason 2 – COPD and Bronchitis
Reason 3 – Heart Attack
Reason 4 – Heart Failure
Reason 5 – Osteoarthritis of the Knee
CIHI. (2021, 04 29). Hospital stays in Canada. Retrieved from Canadian Institute for Health Information.
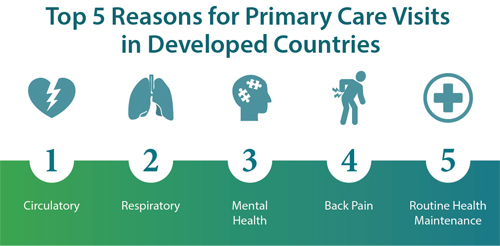
Top Five Reasons for Primary Care Visits in Developed Countries
Long description
Reason 1 – Circulatory
Reason 2 – Respiratory
Reason 3 – Mental Health
Reason 4 – Back Pain
Reason 5 – Routine Health Maintenance
Finley, C. R., Chan, D. S., Garrison, S., Korownyk, C., Kolber, M. R., Campbell, S., Eurich, D., Lindbald, A. J., Vandermeer, B., Allan, G. M. (2018). What are the most common conditions in primary care? Canadian Family Physician, 832-840.
-
About the CIHR Institute of Circulatory and Respiratory Health
The Institute of Circulatory and Respiratory Health (ICRH) is one of thirteen virtual Institutes that make up the CIHR, Canada’s premier health research funding agency.
The ICRH activities and investments provide strategic support for the research community within its mandate, strengthens this community’s competitiveness in obtaining other research support from CIHR (as well as other provincial, national and international funding organizations) and fosters capacity development of the ICRH research community across the CIHR research pillars (I - biomedical; II - clinical; III - health systems and policy; and IV - population and public health) (1), while addressing equity, diversity and inclusion (EDI) and support across all career stages.
The ICRH Institute Advisory Board (IAB) further supports these actions by providing advice on the Institute’s strategic directions and priorities. The IAB includes individuals with lived and/or living experience, as well as scientific and policy experts from across Canada who represent the diversity of sex, gender, race, career stage, regions and research areas encompassed within the ICRH mandate.
The Mission of ICRH
The mission of ICRH is to be an active and meaningful contributor to the collective goals of CIHR by supporting the research community within its mandate and to continue to advance Canada’s position as a leader in addressing circulatory and respiratory health and wellness challenges for all people living in Canada.
The Mandate of ICRH
The mandate of ICRH is broad and supports research into the causes, mechanisms, prevention, screening, diagnosis, treatment, support systems and palliation for a wide range of conditions associated with the heart, lung, brain (stroke), blood vessels, blood, critical and intensive care, sleep and circadian rhythm.
ICRH Values
Excellence and Leadership: A high level of professionalism and exemplary leadership is expected by the research community. The Institute is committed to excellence and leadership in supporting circulatory and respiratory health research and innovation in Canada and throughout the world.
Commitment to Collaboration: The health research ecosystem is dynamic, with many organizations and individuals playing important roles to support health research. The Institute is committed to meaningfully consulting and engaging with our colleagues, partners and stakeholders.
Respect for People: Health research is most impactful, more robust and generalizable when everyone is included. The Institute is committed to supporting the principles of equity (fairness), diversity (representation) and inclusion (valued participation) in all interactions and across all aspects of ICRH's daily operations.
Integrity and Accountability: Health research needs to meet the highest international standards of excellence and integrity. The Institute is committed to decision-making based on evidence, accountability and transparency.
-
The Scope of the ICRH Mandate
The burden of disease covered by the ICRH mandate is significant, encompassing numerous areas related to cardiovascular and respiratory health, stroke, sleep and circadian rhythm, blood and blood vessels and critical care sciences.
Research advances to address the burden of circulatory and respiratory diseases have been significant; however, much work remains as the global prevalence of cardiovascular and respiratory diseases continue to rise.
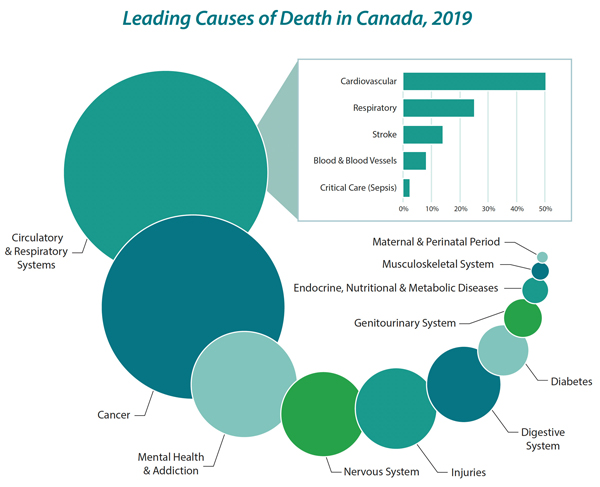
While malignant neoplasms remain the single most common cause of death in Canada, cardiovascular disease is a close second. The full spectrum of health conditions covered by the ICRH mandate (e.g., cardiovascular and respiratory) represent a staggering 42% of all deaths in Canada (2).
In addition, three of the five leading causes of hospital admission in Canada result from circulatory and respiratory diseases (e.g., heart failure, heart attacks and chronic obstructive pulmonary disease [COPD] and bronchitis) (3).
Many of these conditions present frequently for ambulatory care assessment within emergency departments and primary care (4). In summary, presentations of patients with the various conditions contained within the ICRH mandate account for a large burden on society and on the acute care system.
In Canada, one in three adults lives with at least one chronic disease. An estimated 2.4 million people live with ischemic heart disease, 2.1 million are living with COPD (one of the most common types of chronic respiratory disease) and 800,000 are living with the effects of a stroke (5).
The lifetime risk for developing hypertension among adults aged 55 to 65 years with normal blood pressure is 90% and more than one in five adults aged 20 years or older are living with diagnosed hypertension, while an estimated 17% are not aware they have the condition (6,7).
Notably, circulatory and respiratory diseases account for two of the ten leading causes of death in Canada (2). Clearly, there is a significant economic cost associated with circulatory and respiratory conditions.
Demographics (age, race, ethnicity, sex and gender), environment (air pollution) and lifestyle (smoking, diet, exercise, and sleep) all contribute to an increased risk for circulatory and respiratory diseases. The number of people living with a chronic disease, such as heart and chronic lung disease, increases with age and with the growth of the Canadian population. Not surprisingly, these numbers are increasing.
Circulatory and respiratory conditions disproportionately affect Indigenous Peoples (First Nations, Inuit and Métis) and racialized communities living in Canada (8,9,10).
Circulatory and respiratory conditions also affect males and females differently. For example, ischemic heart disease symptoms present differently in women when compared to men and there are sex and gender specific risk factor differences for cardiovascular diseases (11).
More than 20% of all cardiovascular deaths globally are caused by air pollution; and environmental air pollution is one of the most important risk factors for circulatory and respiratory diseases (12).
Canada continues to have a high prevalence of modifiable lifestyle factors such as inactivity, poor sleep, unhealthy eating and harmful use of alcohol, with 85% of adults in Canada reporting to having at least one of these risk factors. More recently, disrupted sleep is on the rise as a result of the ongoing COVID-19 pandemic further contributing to the risk of circulatory and respiratory conditions (13).
There is also a significant economic cost associated with circulatory and respiratory conditions as these represent a considerable proportion of emergency department visits, hospital admissions and critical care utilization. For example, presentations of chest pain, COPD, heart failure and sepsis consume important health resources and contribute to over-capacity within the health care system.
Finally, hypertension is the most common reason to visit a doctor, the number one reason for taking medication and significantly increases risk for stroke, ischemic heart disease, peripheral vascular disease and heart failure.
Leading Causes of Death in Canada 2019
Long description
Leading Cause of Death (Descending Order) Percentage of Total Deaths Circulatory and Respiratory Systems 37.0% Cancer 29.6% Mental Health and Addiction 10.9% Nervous System 5.5% Injuries 5.4% Digestive System 4.6% Diabetes 2.6% Genitourinary System 2.3% Endocrine, Nutritional and Metabolic Diseases 1.1% Musculoskeletal System 0.8% Maternal and Reproductive 0.4% Leading Cause of Circulatory and Respiratory Systems (Descending Order) Cause Percentage of Total Deaths Cardiovascular 50.2% Respiratory 25.4% Stroke 13.6% Blood and Blood Vessels 8.6% Critical Care (Sepsis) 2.1% Statistics Canada. (2022, 01 27). Deaths, 2019. Retrieved from Statistics Canada. (2022, 01 27). Deaths, 2019.
-
The ICRH Research Community
Canadian contributions to research advances that address circulatory and respiratory disease are significant, and many Canadian researchers are recognized as international research and thought leaders. The circulatory and respiratory health research community has consistently been highly ranked for its size, making major advancements and discoveries to address the health and wellness of individuals locally, nationally and internationally (14).
The Institute has a responsibility to provide strategic supports to attract and retain this vibrant research community as well as a duty to advance all research communities within its mandate. ICRH also has a commitment to incorporate the principles of EDI in supporting its research community across the CIHR research pillars for ongoing advancement of health equity, generation of new evidence and knowledge mobilization (KM).
Creating the right balance of support across such varied research communities within the ICRH mandate continues to be at the core of our strategic efforts. The collective effort of the community within and beyond the Institute mandate are paramount to reducing the burden of circulatory and respiratory diseases and is critical to building a more resilient, equitable and healthier Canadian society.
-
Effects of the Global Pandemic
The ongoing direct and indirect effects of the global COVID-19 pandemic have further contributed to the high prevalence of circulatory and respiratory conditions in Canada, and around the world (16). Clearly, the COVID-19 infection is a respiratory condition, which can lead to hospitalization and need for critical care services. In addition, people with pre-existing circulatory and respiratory conditions are at greater risk of severe illness and death resulting from COVID-19 infection. During the pandemic, venous thromboembolism, neurological and sleep-related disorders have also been prevalent (13,17,18)
The COVID-19 pandemic has also brought unprecedented challenges, and in some cases opportunities, for the ICRH community, its partners (including patients), and colleagues. The pandemic has, however, mainly been challenging for many of our partners and colleagues and we understand there is uncertainty regarding the immediate future. As part of the strategic planning process, ICRH consulted with its broader membership (both organizations and individuals), with a specific focus on their experiences related to the COVID-19 pandemic.
Consequently, our near- and medium-term actions will focus on the Institute and community’s shifting context since the pandemic began and its implications into the future. The Plan aims to both maximize the opportunities presented by the COVID-19 pandemic and respond to its related challenges, while also remaining flexible as its true impacts become better quantified and understood.
-
Alignment to the CIHR Strategic Plan
The Institute shares responsibility for achieving CIHR's Strategic Plan (2021–2031) that has a bold Vision for a Healthier Future to encourage Canadian researchers to think in the broadest possible terms about how they can demonstrably improve the health of people in Canada and throughout the world (15).
While the ICRH Plan directly aligns with CIHR’s overall strategic plan, the identified Institute strategic priorities and foundational themes are specific to the needs and interests of the ICRH research community, people with lived or living experience (PWLE) and partners. ICRH adopted CIHR’s corporate values as its own and will apply these values in how The Plan will be actioned.
-
Performance Metrics and Evaluation
The Institute is committed to the continuous monitoring and assessment of the strategies to measure progress of the three strategic priorities and two foundation themes throughout the period of The Plan. To guide this, the Institute will convene a subcommittee that is specifically tasked with developing a performance measurement framework with indicators to complement this strategic plan and leverages CIHR’s Performance and Outcome Measurement Framework. The performance measurement framework will be evergreen and internal, which the Institute will maintain and modify on an annual basis as needed. Ongoing support to the performance measurement framework will be provided by the IAB, input from relevant CIHR staff, and in collaboration with the CIHR Planning, Evaluation and Results branch, as required.
-
Works Cited
- Government of Canada, Canadian Institute of Health Research. (2018, 03 28). Retrieved from The Four Themes of CIHR Funded Health Research
- Statistics Canada. (2022, 01 27). Deaths, 2019 Retrieved from Statistics Canada
- CIHI. (2021, 04 29). Hospital stays in Canada. Retrieved from Canadian Institute for Health Information
- Finley, C. R., Chan, D. S., Garrison, S., et al. (2018). What are the most common conditions in primary care? Can Fam Physician, 832-840.
- Branchard, B., Deb-Rinker, P., Dubois, A., et al. (2018). At-a-glance How Healthy are Canadians? A brief update. Health Promot Chronic Dis Prev Can, 385-390.
- Hypertension Canada. (2016, 05). Retrieved from Hypertension in Canada
- Government of Canada, Public Health Agency of Canada. (2010, 07 22). Retrieved from Hypertension Facts and Figures
- Kovesi, T. (2012). Respiratory disease in Canadian First Nations and Inuit children. Paediatr Child Health, 376-380.
- Anand, S. S., Abonyi, S., Arbour, L., et al. on behalf of the Canadian Alliance for Healthy Hear. (2019). Explaining the variability in cardiovascular risk factors among First Nations communities in Canada: a population-based study. Lancet Planet Health, E511-E520.
- Chiu, M., Austin, P. C., Manuel, D. G., et al. (2010). Comparison of cardiovascular risk profiles among ethnic groups using population health surveys between 1996 and 2007. CMAJ, E301-E310.
- Norris CM, Yip, C.Y.Y., Nerenberg, K.A., et al. (2020). State of the Science in Women's Cardiovascular Disease: A Canadian Perspective on the Influence of Sex and Gender. J Am Heart Assoc, e015634.
- Brauer, M., Davaakhuu, N., Escamilla Nuñez, M., et al. (2021). Clean Air, Smart Cities, Healthy Hearts: Action on Air Pollution for Cardiovascular Health. Global Heart.
- Alimoradi, Z., Broström, A., Tsang, H. W, et al. (2021). Sleep problems during COVID-19 pandemic and its’ association to psychological distress: A systematic review and meta-analysis. EClinicalMedicine, 2589-5370.
- Government of Canada, Canadian Institutes of Health Research. (2021, 04 27). Retrieved from Review of the Institute of Circulatory and Respiratory Health (ICRH)
- Government of Canada, Canadian Institutes of Health Research. (2021, 02 23). Retrieved from CIHR Strategic Plan 2021-2031
- Kaczorowski, J., & Del Grande, C. (2021). Beyond the tip of the iceberg: direct and indirect effects of COVID-19. Lancet Digit Health, e205-e206.
- Marshall, M. (2021). COVID and the brain: researchers zero in on how damage occurs. Nature, 484-485.
- McBane, R. D. (2020). Thromboembolism and the Pandemic. J Am Coll Cardiol, 2073-2075.
- Collins, J. (2001). Good to Great: Why Some Companies Make the Leap...And Others Don't. London: Random House.
- Graham, I. D., Logan, J., Harrison, M. B. et al. (2006). Lost in knowledge translation: Time for a map? J Contin Educ Health, 13-24.
- Statistics Canada. (2022, 02 02). Data products, 2016 Census. Retrieved from Statistics Canada
- Government of Canada. (2022, 03 24). The 50-30 Challenge: Your Diversity Advantage. Retrieved from Innovation, Science and Economic Development Canada
-
Appendices
Appendix 1: Acknowledgments
Institute Advisory Board

P.J. Devereaux, MD, PhD, FRCPC (Chair)
Director, Division of Perioperative Care
McMaster University
Tier 1 Canada Research Chair in Perioperative Care
Marilyn MacKay-Lyons, Professor, School of Physiotherapy
Dalhousie University
Affiliated Scientist, Nova Scotia Health
Sucdi Barre, BA
Patient with Lived Experience,
Wellness Coach
Liam R Brunham, MD, PhD, FRCPC, FACP, FNLA
Assistant Professor and Canada Research Chair,
Department of Medicine, Centre for Heart Lung Innovation
University of British Columbia
Elaine Chong, BSc (Pharm), ACPR, PharmD, FCSHP
Director, Health Program Integrity and Control Migration Health Immigration,
Refugees and Citizenship Canada
Shurjeel Choudhri, BSc (med), MD, FRCPC
Senior Vice President and Head,
Medical and Scientific Affairs Bayer Inc.
Catherine L. Cook, MD, MSc, CCFP, FCFP
Vice President (Indigenous) at the University of Manitoba
University of Manitoba
John Fleetham, MD, FRCP
Professor of Medicine
University of British Columbia
Susan Kahn, MD MSc, FRCPC
Professor of Medicine, Canada Research Chair,McGill University
Director, JGH Centre of Excellence in Thrombosis and Anticoagulation Care (CETAC)
François Lamontagne, MD, MSc, FRCPC
Full Professor, Université de Sherbrooke
Clinician scientist, Centre de recherché du CHU de Sherbrooke
Melissa J. Parker, MD, MSc, FRCPC, FAAP
Associate Professor of Pediatrics
McMaster University
Grace Parraga, PhD, FCAHS
Tier 1 Canada Research Chair and Professor
Division of Respirology, Department of Medicine; Department of Medical Biophysics
Western University
Andrew Pipe, CM, BA, MD, LLD (Hons), DSc (Hons)
Clinician-Scientist, University of Ottawa Heart Institute
Professor, Faculty of Medicine
University of Ottawa
Rita Suri, MD, MSc, FRCPC
Director, Division of Nephrology, McGill University
Director, Division of Nephrology, McGill University
Scientist, Research Institute of the McGill University Health CenterPartner Advisors
Charities
Canadian Allergy, Asthma, and Immunology Foundation
- Andrea Waserman
Managing Director
Canadian Lung Association
- Terry Dean
President & Chief Executive Officer (CEO)
Cystic Fibrosis Canada
- Paul D.W. Eckford, PhD
Program Director, Research
Heart and Stroke Foundation of Canada
- Diego Marchese
Executive Vice President, Mission, Research and Social Enterprise - Mary Elizabeth Harriman, MBA Director, Research and Partnerships
Societies
Canadian Cardiovascular Society
- Carolyn Pullen, PhD
Chief Executive Officer (CEO) - Marc Ruel, MD, MPH, FRCSC, FCCS
President
Canadian Critical Care Society
- Bojan Paunovic, MD, FRCPC
Past President - Claudia C. dos Santos, MSc, MD, FRCPC
Scientific Chair
Canadian Sleep Society
- Célyne Bastien, PhD
President - Thanh Dang-Vu, MD, PhD
Vice-President (Research)
Canadian Society for Atherosclerosis, Thrombosis and Vascular Biology
- Scott P. Heximer, PhD
Past President
Canadian Thoracic Society
- Janet Sutherland
Executive Director - Paul Hernandez, MDCM, FRCPC
President
Hypertension Canada
- Ross T. Tsuyuki, BSc(Pharm), PharmD, MSc, FCSHP, FACC, FCAHS, ISHF
President - Asif Ahmed
Executive Director
Thrombosis Canada
- James D. Douketis, MD, FRCPC, FACP, FCCP, FCAHS
Past-President
Government
Healthcare Excellence Canada
- Jennifer Zelmer, PhD
President and Chief Executive Officer (CEO)
National Health Lung and Blood Institute (NHLBI), NIH
- David Goff, MD, PhD
Director, Division of Cardiovascular Sciences - James Kiley, PhD
Director, Division of Lung Diseases
PHAC, Health Promotion and Chronic Disease Prevention Branch
Industry
AstraZeneca Canada
- Andrew Foster, PhD
Medical Advisor - Mena Soliman, MD, MSc
Scientific Director – Respiratory & Immunology Medicines
Community Roundtables
Participants of the virtual focus group sessions centered on one of the following themes:
- Enhancing Equity, Diversity and Inclusion
- Strengthening Indigenous Health Research
- Accelerating Knowledge Through Collaboration
- Preparing for the Future
- Patients and People with Lived/Living Experience
Participants (Name, Affiliation [if applicable])
- Ejaife Agbani, University of Calgary
- Samira Chandani, Patient/Caregiver
- Thanh Dang-Vu, Concordia University
- Kerstin de Wit, Queen's University
- Heather Dyck
- Heather Foulds, University of Saskatchewan
- Vivek Gill, CIHR Institute of Human Development, Child and Youth Health (CIHR-IHDCYH) Youth Advisory Council
- Jordan Guenette, University of British Columbia
- Padma Kaul, University of Alberta
- Malcolm King, University of Saskatchewan
- Manoj Lalu, Ottawa Hospital Research Institute
- Kent Cadogan Loftsgard, CIHR/SPOR
- Sunny Loo, Patient Partner, Michael Smith Health Research BC
- Donna Martin, University of Manitoba
- Farah Mawani, York University; and MAP Centre for Urban Health Solutions, Unity Health Toronto
- Asher Mendelson, University of Manitoba
- Eki Okungbowa, CIHR Institute of Human Development, Child and Youth Health (CIHR-IHDCYH) Youth Advisory Council
- Gavin Oudit, Department of Medicine, University of Alberta
- Mireille Ouimet, Ottawa Heart Institute, University of Ottawa
- Sara Pintwala, University of Toronto
- Michelle Ploughman, Memorial University of Newfoundland
- Rithwik Ramachandran, University of Western Ontario
- Kristine Russell, Sepsis Canada
- Anni Rychtera, BC SUPPORT Unit
- Min Hyung Ryu, Brigham and Women's Hospital, Harvard Medical School
- Georg Schmölzer, University of Alberta
- Nariman Sepehrvand, Department of Medicine, University of Alberta
- Swapnil Shah
- Mike Warren, NL SUPPORT Unit
- Zoe White, University of British Columbia
- Rita Wiebe
- Bilqis Williams, OSSU SPOR
- Amy Y. X. Yu, University of Toronto
Institute Staff
- Kaylin Barnes, BEd
Lead – Communications and Events - Helen Coe, PhD
Lead – Institute Initiatives and Partnerships - Ryan Perry, PhD
Associate Scientific Director - Brian H. Rowe, MD, MSc, CCFP(EM), FCFP, FCCP, FCAHS
Scientific Director - Ebele Unaegbunam, MSc
Project Lead – Strategic Initiatives
Contributors
- MP Strategy Group (MPSG; Michel Perron, Michelle Gagnon, Erika Beresford-Kroeger)
- Indigenous Health Research Team, CIHR Initiative Management and Institute Support Branch (Pascale Bouffard, Initiative Officer; Samantha Fauteux, Associate; Jenna Ives Project Lead, Major Initiatives)
- Graphic Designer: Kyle Loranger Design Inc. (Kyle Loranger)
- Illustrator: Kate Campbell Medical & Scientific Visualizations (Kate Campbell)
Appendix 2: The ICRH Strategic Planning Process – Methods
As part of The Plan development, ICRH undertook a meaningful and thorough consultation process with key partners, researchers and the broader community.
The purpose of the consultation process was to ensure that The Plan considered the threats, opportunities and challenges faced within the ICRH community in a post-pandemic context.
The Institute retained MP Strategies Group (MPSG) to support the strategic planning process and helped co-develop six lines of inquiry. These lines of inquiry were used to guide key partner interviews, IAB discussions, community engagement sessions and an online community consultation (survey).
The lines of inquiry were also used to collect input from key partners and community members on proposed priorities and provided a validation on their relevance and resonance in guiding future actions. In addition, the lines of inquiry were designed to identify collaboration options with partners, as well as to uncover new or unrecognized alternate priorities for consideration. The inquiry involved seeking input from those who spoke on behalf of organizations, as well as those who spoke from the perspective of an individual with lived or living experience.
Results of the lines of inquiry were collated into a “What We Heard” report, which summarized input on the proposed strategic priorities, as well as identified gaps, threats and opportunities faced by the ICRH community. Information from the “What We Heard” report was used to develop the central tenet, the three strategic priorities, the two foundational themes and associated strategic actions for The Plan. This was then presented to the IAB to provide feedback and advice to support the final development of The Plan.
Partner Engagement Interviews
Between August and October 2021, MPSG and ICRH each led interviews with key partners. Key partners were defined as those having a partnering history with ICRH and/or alignment with ICRH mandate areas. Interviews included representatives from organizations such as charities and societies, who were asked to speak on behalf of their organization as a collective. MPSG undertook ten virtual interviews and ICRH undertook three virtual interviews. Where possible, ICRH IAB members attended meetings as observers to enable provision of ongoing strategic and expert advice to ICRH.
Online Consultation (Survey)
In order to engage the broader ICRH community, a REDCap (Vanderbilt University, Nashville, TN) survey was developed to collect demographic and key feedback (both quantitative and qualitative). The survey was launched in early September 2021, to collect responses over one month. The survey was disseminated through the ICRH communication channels, to key partner groups identified for engagement and to ICRH IAB members for amplification through their networks. There were 103 respondents to the survey. The survey captured perspectives from individuals, rather than those representing organizations.
Community Roundtables
In October 2021, feedback was also solicited from a broad range of community members through ten virtual focus group sessions centered on one of the following themes:
- Enhancing Equity, Diversity and Inclusion;
- Strengthening Indigenous Health Research;
- Accelerating Knowledge through Collaboration;
- Preparing for the Future; and
- Patients and People with Lived/Living Experience.
Two meetings per theme were organized with no more than six participants at each meeting to permit participant dialogue. The sessions encouraged community members to provide perspective and practical ideas on how ICRH might mobilize its strategic priorities within each area. Meetings were facilitated by ICRH with ICRH staff, an IAB member and a member of MPSG attending as observers.
ICRH Institute Advisory Board Engagement
In addition to input provided during IAB meeting points, MPSG facilitated two focused virtual group discussion sessions with IAB board members in August 2021. Conducted in alignment with the partner engagement interviews, these discussions followed the six lines of inquiry. Notes from all discussions were captured by facilitators for later use in the development of The Plan.
CIHR Approval Process
The Plan was reviewed internally by Dr. Sarah Viehbeck, Associate Vice-President Research – Evidence Integration, Dr. Michelle Peel, Acting Associate Vice-President Research – Evidence Integration and Ms. Erin Dunn, Senior Advisor to the Associate Vice-President / Research Programs - Strategy at CIHR. Furthermore, The Plan was reviewed at Science Council in February 2022, underwent iterative review by CIHR in March 2022 and received approval in April 2022 from Dr. Michael Strong, President - CIHR. The Plan was released in May 2022.
- Andrea Waserman
- Date modified: